Chapters
Transcript
[MUSIC PLAYING]
CURT DANIELS: I hope to give you a feel for adult congenital heart disease, overall, and how we take care of patients today in 2019 and 2020. I'll talk a little bit about our program, And then towards the end we'll go through some interesting challenging cases that we deal with almost on a weekly basis so you get a little feel for that.
So let's talk about the congenital heart disease population. And I'm going to start with what I call ground rules, so this is Chicago, Wrigley Field and baseball, you have to go through the ground rules at every stadium. It's different than any other sport, there's ground rules per stadium. And so for congenital heart disease my ground rules are to talk about how we describe severity. And forever, and ever, and ever, that I recall, we've always described the severity of congenital heart disease based upon your birth anatomy, so what you were born with actually defined the severity.
And I'm going to go through a little bit of that. So there's mild disease, and mild disease can be things like ASDs and ASDs that are closed. Moderate disease has a large list, it's our largest list, Ebstein's anomaly, coarctation, Tetralogy of Fallot, for example. And then we have those with severe disease. Probably the most common, at least concerning that we see, is a single ventricle Fontan patients right here. And so that's how we've always defined severity, but I'm going to show you a new way in which we think about severity of congenital heart disease today, not just looking at anatomy but looking at other factors, and I'll get to that in a little bit.
So if we look at survival, making it to 18 years of age through the decades, in the 1940s you had about a 20% chance of making to adulthood, because there really wasn't much back then, there was the Blalock-Taussig shunt and that was about it. 1940 and 1960s, we moved into open heart surgery, moving into the heart and repairing the heart. But by the 1970s, when the surgeons started doing neonatal surgery, repairing early, we began to see improvements of overall survival, 75%, 80%, and 90%. This has really changed the epidemiology of congenital heart disease.
The red boxes are adults, the blue are children. And you can see over time, we now have more adults than children with congenital heart disease, by a 2/3 margin. So congenital heart disease really as an adult phenomenon more than a pediatric phenomenon today in terms of population analysis. And this is really related to the prevalence of those with severe disease now surviving. So in the past those with real severe disease did not make it to adulthood, and now we're seeing that at a much, much greater rate, and that's really changing the trajectory of the congenital population.
So today we say 90% of those born with congenital heart disease are expected to make it to adulthood, and this has created tremendous success. This is success, success from pediatric cardiology, cardiothoracic surgery, all of those deserve the credit for getting children to adulthood. But I say with great success comes great responsibilities and great challenges, and this patient population is a great challenge from those successes of the past coming towards us.
I give an example here, success of a population. I think 20 years ago we would not have thought about putting ICDs in 85 and 90-year-olds, but today patients are living longer. And so we have a success of patients living longer, now, we think about putting ICDs in older patient population.
So as a correlate, in our patient population, success has led to many challenges, arrhythmias, all types of arrhythmias, heart failure, every type of heart failure that we have is rolled into the adult congenital patient that we see. They have vascular lesions, residual shunts, aortic disease, valvular heart disease and extracardiac disease. I'll touch on some of these.
And this has changed the risk for these patients, their morbidity is two to three times higher than people their own age. 20, 30, and 40-year-olds shouldn't be in the hospital with heart disease, and so with their risk and all the complications they have, they're in the hospital much more often than their cohorts compared to a normal Quebec population in this study. And also, their mortality is significant.
And so in this particular study from the Netherlands of about 7,000 patients, the mean age of death was 30. And so if we said, gosh, we're going to do all this work to get them to adulthood but your mean age of death is 30, that's obviously super concerning when you look at the overall risk for this patient population, with arrhythmias and heart failure being almost half of that mortality overall. And almost across the board, every congenital lesion you see here has a higher risk than the general population. All the way from ASDs, even a small change, to down to Fontans, with a 20 times risk compared to people their own age of mortality.
If you want to look at it a different way, in this large UK study of about 6,000, 7,000 patients, if you look at a risk of five-year mortality and you say if you're a 40-year-old what is your equivalent age for a 40-year-old with congenital heart disease, for Tetralogy of Fallot it would be a 50-year-old. So when I'm seeing a 40-year-old in clinic with Tetralogy of Fallot they have an equivalent risk of death as a 50-year-old without heart disease. And how about Fontan patients? 75-year-old. So if I'm looking at a 40-year-old Fontan patient, they have equivalent risk of death of a 75-year-old. So again, I think sometimes we don't think about that when we see our patients in clinic.
So they have a lot of-- a number of long term complications. Survival is not as expected, heart failure and arrhythmias are concerning, morbidity is certainly substantial. But then we also have adult comorbidities, and this is the challenge as well as the patient population ages. They do have coronary disease, and diabetes, and obstructive sleep apnea, and end organ disease.
As an example, a 38-year-old that came into the hospital here with tetralogy of flows repaired, has diabetes and came in with chest pain. And you can see at the top of the picture there is a stent up here, a stent up here for pulmonary stenosis. And then you can see this tight 90% corneal lesion. So sometimes if we're just focused on the congenital heart disease we can forget the big picture of our patient population.
Let's talk about electrophysiology just a little bit. Our patient population has a huge amount of atrial arrhythmias. This is a large study, 482 patients, at least in our field, 12 centers got together and did this study. What it basically shows that IART is significant, and it increases depending on the severity of your disease. The red boxes are IART, and you can see it goes up as complexity of disease goes up. But as the patient population ages, just like anything else, we see more AFib. And so they have atrial fibrillation, they have IART, which is substantial.
If you look at the atrial arrhythmia risk, a 20-year-old with congenital heart disease has an atrial arrhythmia risk equivalent to a 55-year-old without congenital heart disease. So again, we're shifting all this risk to a younger population. A Fontan looks like a 75-year-old. A 20-year-old looks like a 55-year-old when you look at atrial arrhythmia risk. And once you have atrial arrhythmias your risk of mortality is up 50%, stroke 50%, heart failure, 2 and 1/2 times greater.
Let's look at some specific examples of patients that we see. So here's transposition of the great arteries, and some of our patient population have an atrial switch, a big baffle in the middle, up in the atria. And so here's a 25-year-old with d-transposition Mustard who had syncope while driving and came to a local hospital. And you can see here, this doesn't look good. This is our local hospital up here, Bellfontaine, not far from here. And you see P, QRSes, P, QRSes, and then just P waves, not good.
And so placing pacemakers in this patient population is not easy, it's complex. You have to course-- you have to course through the baffle. You have to place this one in a left ventricle, which is the subharmonic ventricle, and many times they're obstructed. And so this vein is completely obstructed, you can see the pacemaker sitting on the chest because they couldn't get the pacemaker in. There's no way to course through this here, and so many times we have to place a stent ahead of time. So here's a stent, then the pacemaker leads are placed after that.
Here's a 36-year-old with d-transposition Mustard, palpitations, near syncope, and has atrial tachycardia, but then also the same patient has ventricular tachycardia. And so we see complex arrhythmias rolled up into one particular patient And performing interventions on this population is not easy, we have a systemic venous baffle, a pulmonary venous baffle you have to deal with, and it's much more complicated.
And so in this particular patient I'll show you, Dr. Kalbfleish, who's an adult electrophysiologist, worked with Dr. Kamp, who's a pediatric electrophysiologist, who worked with our congenital interventionalist to perform this procedure. Because what they had to do is they had to course through this baffle. And so there's the baffle. This is an injection in the SVC, and you can see the flow through the baffle up there at the top. And so they did an angiographic overlay, which is this, and had to poke through the baffle.
So here's the catheter poking through the baffle right here, with a little needle at the end of the catheter poking through to get to the other side. And this is, you can see, sort of poking through right there. And so then the electrophysiologist could put their catheter in there and do their ablation procedure. So it took a team approach for this one procedure. It wasn't as simple as go to the EP lab and let's form an atrial ablation is as we might do another patients.
We also see sudden cardiac death for our patient population. Again, in a large Netherlands study I drew a line at 40 years of age, and look at all the lesions that have a risk of sudden cardiac death less than 40 years of age. So again, this is a major issue, and I'll talk about what we need to do for the future.
Coarctation, as an example, for vascular disease, you see multiple ways in which you can fix coarctation. And so in our world, if we hear coarctation, the next thing we want to know is how was that fixed. Because it matters how it's fixed, you can have pretty straightforward aortic arches, or you could have one that looks like this. This is one of my patients, a very complex arch, very hard to figure out what's going where in that picture. A number of bypass grafts have been done.
Here's a 34-year-old with a repaired coarct, hypertension for 14 years. Now the LVF is 20%, and the first time anybody took a look at the arch it was completely disconnected where she had previously had that repaired, and now it's completely disconnected. We did a study a few years back and we looked at patients, and we asked the question, if we did screening arch imaging, what would be find? Patients who had normal echos, no symptoms, if we just looked at the arch in a regular basis, what would we find? And we found that about half of the patients we had we found significant abnormalities.
Here's one of the patients from that study. This is the first time this arch was looked at since surgery, and this is 35 years ago. And there's a localized dissection right there. You can't see these with echocardiography most of the time, that's what our study showed. Here's a 25-year-old screening study, again, big aneurysm. There's another screening study we did, here's a pseudoaneurysm.
And these are important to find, because these are risks for vascular complications and sudden death. And we can place a covered stent and exclude those aneurysms. So a fairly straightforward simple procedure can actually relieve the risk of somebody having a vascular complication.
Here's somebody who had a stent placed seven years ago and had no follow up studies, has a big pseudoaneurysm pushing through that stent. That's not a covered stent, it's an uncovered stent. So our guidelines try to reflect some of this information. And so we know then, coarctation, they're at risk. They're at risk for aortic complications. And so our guidelines today say that you should do initial and follow-up imaging of the aortic arch with CT or MRI.
They also have aortopathies as well. Here's a patient we reported on who's a Fontan patient, the first ever reported to have an aortic dissection. You can see the dissection plane right there. An adult congenital cardiologist from Japan, Koichiro Niwa, wrote about the number of patients who have had dissections with adult congenital heart disease over the years. You can see very large aortas, a number of different diagnoses.
I used Tetralogy of Fallot as an example of valvular heart disease. We see pulmonary insufficiency in the majority of these patients. There's the right ventricle, pulmonary artery. The majority of them have their pulmonary valve intervened on as children, as infants, and so they end up with severe pulmonary insufficiency, which we see.
This is a complex set of diseases because these patients, many times, have had multiple surgeries. Open heart surgery is the typical way to replace a valve, we know that. Think about your adult patients, when they go to the operating room many times it's their first open heart surgical procedure. But in our patients, it may be their second, third, fourth, or fifth.
This is a study from Italy, it looked at morbidity and mortality related to surgical operations, and the more interventions, the more surgical procedures you have, the more sternonomies, the higher the risk is, more morbidity, more mortality. And our population, by the time they get even to 20 or 30 years of age, it might already be their second, third, or fourth surgery. Again, that's a risk, so how can we change that trajectory for those patients?
So I talked about the mortality, and heart failure is a big one, and we see multiple types of heart failure. Here's again another patient D-TGA, atrial switch, RV ejection fraction of 32%. And this is a complex problem for us because we don't have a lot of data. We see single ventricle Fontan patients. This is an old Fontan we'll call it, because it's the way it was connected. You can see the flow through there is not so great, so how can someone even walk around and survive with something like that? That's a single ventricle Fontan.
And we know now there's multiple types of what we call Fontan failure. If you look over here to the side, there's many factors that can lead to Fontan failure. So now we describe four different basic phenotypes of Fontan failure. It's not all just the Fontan fails, the heart can fail, pulmonary vascular disease can be a part of it, systemic vascular disease can be a part of it.
So what is the circulation physiology of a Fontan patient? I'm going to talk about this now and a little bit more towards the end. So a normal circulation, your right atrial pressure can be very low, and the venous pressure can be very low, because you have a pump, you have a right ventricle that actually pumps blood into the pulmonary circulation. It can overcome the resistance in the circuit by having a pump.
In a Fontan circulation, you do not have a pump on that side, there's no right-sided pump. And so you have high right atrial pressure. As soon as that Fontan is hooked up in a one-year-old, there's elevation of the venous pressure right away. It would go from a normal of five to probably somewhere around 12 to 13 as soon as things are hooked up because there's no pump on that side.
And so depending upon your Pa pressure, or resistance I should say, your left atrial pressure, LVDP then, over time, you can have higher, and higher, and higher Fontan pressures in order for blood to flow, circulation to flow. And this has led to issues related to, I'll call extracardiac disease. So the Fontan population have a series of extracardiac disease, one of which is liver disease.
And so here is a patient with a Fontan, a slightly different type of Fontan than I showed you a minute ago. And in this population they have elevated pressure within their Fontan itself, this is driven by LVDP and driven by pulmonary vascular disease, there's a pulmonary vascular bed. This leads to high pressure in their IBC, hepatic veins, and inside the liver itself.
So in every area of the liver you have elevated pressure inside of the liver itself. This also leads then to portal pressure, it's all connected together. And so right from the get go, patients, babies, children, have portal pressures instead of being five, six, seven, now, of 10, 11, 12, 13 from the time their initial Fontan is hooked up.
And so we put together a conference a few years back to try to define this liver disease. We were seeing it in all patients, and we defined this as Fontan-associated liver disease. Elisa Bradley from our group was one of the co-chairs with us to do this study, and we pulled together people from all over the country to try to help better define Fontan-associated liver disease.
And here's an example, here's a 37-year-old patient with complex anatomy, tricuspid atresia. Had an LVDP of 10, had a wedge a 10, had a pulmonary artery pressure, mean pressure of 19, Fontan pressure 19, estimated portal pressure of 21. And already had cirrhosis at age 37.
But go back 20 years earlier, here's a 17-year-old patient, same diagnosis, tricuspid atresia Fontan. Has a wedge at 10, a Fontan pressure says 16, and then has a portal pressure estimated to be 19. And already has an abnormal liver, has evidence of varices, and already has significant fibrosis at age 17. So liver disease is really ubiquitous in our population.
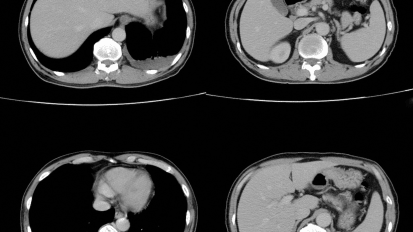
Here's a patient recently that we've been seeing, and an unfortunate patient. In 2011-- So follow this, in 2011 had a CT scan, CT scan said at the time the liver and the spleen were within normal limits. Go to 2013, two years later, now it's abnormal, it's a heterogeneous pattern of the liver itself. 2014, a year later after that, now it's lobulated and there's suspicion of cirrhosis. Again, this is 2014.
And then really didn't have another study for the next five years, lost a care and some other issues. It's an AFP that's 4,900. Has a CT scan at that time that shows numerous vascular lesions consistent with hepatocellular carcinoma. So that's the possible end result of having cirrhosis. For any patient, having carcinoma is the end result.
So now this has been described in Fontan patients. There's a case series of 33 patients having hepatocellular carcinoma after Fontan operation. So extracardiac disease is a serious problem for our patient population. For the Fontan patients, it's quite concerning.
You go back to heart failure for a second, you know, there really are no heart failure trials in adult congenital heart disease. There are trials, but they're not very good. And so this was an evidence review committee that looked at this one particular question, and this comes up quite a bit, are our heart failure medicines effective for people who have a systemic right ventricle, systemic right ventricle? So that could be a Fontan patient with a right ventricle. It could be a d-transposition Mustard patient. It could be a congenitally corrected transposition patient. Do our medical therapies actually help?
And so a committee got together, did an extensive search through the ACC and AHA to ask that particular question. And the conclusions where there's such limited studies in these agents, and using these for systemic right ventricles, that we couldn't provide any conclusion whatsoever that these medicines are actually effective for systemic right ventricles.
But part of it is we don't have good studies, part of it is the studies we have so far have not shown the same effectiveness. And Dr. Sabanayagam and Dr. Bradley from our group have written a really nice review paper, published last year, to talk about some of these concerning issues.
So I'll say success is creating great new challenges for this population. Some of those I just described, really significant challenges for the population. Challenges in, who cares for these patients, how do we care for this complex population? So for years and decades, COCATS, which sets the guidelines for curriculum, basically said to be an adult cardiologist you needed six hours of congenital heart disease lectures, that's it, to be an adult cardiologist, six hours.
And that's how I trained. When I trained as an adult cardiology fellow all you had to have is six hours of lectures, that's it, and then you were obviously a full-fledged board certified adult cardiologist with no training, basically, in congenital heart disease. So we never took this issue serious in terms of the adult congenital population.
We did a study where we looked across the country of who has trained, and how many adult congenital heart disease fellows over about a 25 year period. And we found 63 people had done any type of training. And this training was variable, from less than 12 months to up to two years. It was under really no guidelines. I'll come back to this in a minute.
We also have challenges with how we deliver care, how do we deliver care? It's not just the cardiologist that delivers care, we all work in a heart center, a care system. Heart failure is probably the best example of that, where you have a team of people taking care of patients with a chronic disease, pulmonary hypertension is the same way. So how do we deliver care? It's not just about the cardiologist.
And over the past we really had a tough time defining this. There's clinics throughout the country that are self identified, over 100, that they say they take care of adult congenital heart disease patients. But this has really been under no obligation to meet any kind of a standard. And really extremes of what we call a program, from a clinic to really full, robust programs.
And we have challenges in our care model because we have children's hospitals, adult hospitals. Advantages and disadvantages in those, right? So the children's hospitals are strong in congenital heart disease, but weak in adult medicine. And traditionally, adult hospitals have been weaker in congenital heart diseases, in terms of having the subspecialty care, the technicians, others that need and be necessary to take care of patients, but then obviously very strong in adult medicine. And so adult congenital heart disease needs to bridge these two worlds and really take the advantages of both and bridge those two things together.
So where are we today in terms of the care model? So we were able to successfully get ACGME approval for fellowship training for adult congenital heart disease. And so there's two pathways today, an internal medicine cardiology pathway and a pediatric cardiology pathway. So we're at two years of curriculum in each. There's 21 programs now that have training for ACHD around the country.
We've changed COCATS from the six hours to at least one month. So out of your 36 months it's now not required, strongly recommended. See the wording, it was very hard to even get strongly recommended in there. Part of that is you have to have an adult congenital program to actually do a month. And so many people go and do away rotations, or try to do the best they can where they're at, but it's at least strongly recommended. And here, we require our fellows to do one month.
Also we're successful in getting board certification started, the first board exam was in 2015. And today we have 300 board certified ACHD docs. I say 2018, because an exam is coming up now in 2019, about 200 people will take the next one. So it should be close to 500 board certified after this year, around the country. And then we published guidelines last year, care guidelines which are pretty detailed compared to the previous ones about 10 years earlier.
Now I'll come back to this concept of the ground rules in anatomy. Remember, I said anatomy is how we define severity of disease. So if you had tetralogy of flow you had moderate disease, considered moderate disease the rest your life. So every epidemiologic database puts you in that moderate category depending on your birth anatomy. So we wanted to think of a different way to do this and think about how does physiology play a role in this, because that's actually how we take care of patients, it's their anatomy and their physiology. We call this the AP classification part of the new guidelines.
And so we take that anatomy and then we add in physiology, stages A through D based upon heart failure symptoms, arrhythmias, pulmonary hypertension, residual shunts, things that we actually have data on that show there's a morbidity and potentially mortality risk associated with that. So physiologic classes A, B, C, and D. And so we take these then, we take these lesion specific anatomy and physiology and plug them into tables, part of the guidelines.
And so here's an example of an Ebstein's guideline, where you have patients with Ebstein's anomaly, that same birth anatomy that you've had your whole life, but now you have different physiology. So I'll show three just very, very random examples of patients. First one is Vladimir, and Vladimir has stage B, and you can see the amount of follow up they he needs. The next one is Kim, and you can see the anatomy and the physiology and the amount of follow up. And then the last one is Donald, and you can see the different physiology that this particular patient sort of needs. And so depending on your physiology, depending on your physiology, you would need to be seen more often, have more testing each time.
Let's go back to the programmatic way. So we had this programmatic way of approaching patients, and we said these were all self identified. And then a landmark article was published right around the time all these other things were happening, board certification, training, all these activities were all happening around the mid-2014, 2015. And this landmark article came out from Quebec, from Montreal.
It looked at 71,000 patients followed in 15 adult congenital centers in Canada. And what they found when they looked at those patients, if they were in an ACHD program they had improved survival. And so those patients who actually were in programs had improved survival. You see on the top line red, over time when they followed them.
So then a decision was made, well maybe we should be looking at how we can build programs with some quality to them. And ACHA, which is the Adult Congenital Heart Association patient advocacy, began to build this process. And so there's a steering committee, and after a lot of work, and about 160 cardiologists getting together, and a lot of time, 20 categories, 100 criteria were developed to develop programmatic way of thinking about accreditation.
And it's a robust application and site visit to accomplish this. It was vetted through about 20 organizations, endorsed by many organizations, this process. And then today we have 30 Adult Congenital Heart Disease accredited programs around the country. We should have 40 by this time, probably, next year.
Let me just pause for a second and talk a little bit about our program, since if you come here you'll get to interact with our program on a regular basis. We have what's considered a large program, we have six ACHD cardiologists, and we have a PhD psychologist as part of our faculty, six board eligible or certified cardiologists. We have a very robust team, we have a team at Children's Hospital made up of nurse practitioners, nurses, office staff, a social worker. And then we a robust team here at Ohio State with the same, of nurse practitioners, nurses, and an office staff to help take care of our patients.
We see about 4,000 patients or so a year, growing every single year, you can see over the almost 20 years of having the program. We do lots of outreach around the state of Ohio, there's three campuses, I'll call it, here in central Ohio, Nationwide, Ohio State, and then we just started a North Campus up in Lewis Center. We do lots of outreach, and Saurabh is the workhorse for the outreach. And he travels around the state of Ohio and dumps off the other cardiologists.
And Aarthi goes-- Aarthi Sabanayagam goes to Mansfield and Dayton. And Lauren goes to Dayton. And I go to some of them as well. But the workhorse in the yeoman's work is Sarbs doing a lot of work in outreach. We see about 600 patients in outreach, just in those outreach clinics. And so we're trying to get out to where the patients are.
We have a fellowship program that's in part sponsored by a family. And these are what our fellows have done since graduating from our program, doing some great work all around the country. We publish a lot, this is about 35 articles just in the last year and a half or so that our team has been a part of publishing.
And as a general fellow at Ohio State, coming here, you'd be required to a one month rotation with adult congenital heart disease, both at Ohio State and Children's Hospital. You do outreach in outpatient care, inpatient, spend some time in the Cathlab, imaging. We have a large pregnancy and heart disease program. We have ACHD education we also fold into that month that you would be a part of. And then outside of that month you certainly would be working with our team on the imaging labs, Cathlabs, inpatient services.
So let me just talk a little bit about future, and then we'll go through a couple of interesting cases. Well, the future is that we need to improve the workforce. You know I showed you some numbers earlier, and there's about 2.5 million congenital heart disease patients in the US. About a million are children, about 1.5 million are adults. And if you look at the ratio of providers to patient and patients to providers, it's about one pediatric cardiologist for every 300 pediatric patients. And it's about one adult congenital cardiologist for every 5,000 patients, and that's just in the US alone.
So very, very small, we have outreach problem. You go back to this slide I showed a second ago, you can estimate with some fancy math, epidemiology, about 16,000 adult congenital patients should be in our catchment area where we see patients. 16,000 just in our catchment area, and we're certainly not seeing all those patients.
We need to improve medical and interventional therapies. As just one example, going back to the guidelines for a second, I showed you this slide of sudden cardiac death risks. Out of all the diagnoses we have with congenital heart disease, we only have one diagnosis that we do primary prevention ICDs with, and that's Tetralogy of Fallot, if you meet certain guidelines. All the others we have no idea should we put a primary prevention ICD. Should we put it in if your RV ejection fraction is weak? Should we put it in if you have a systemic right ventricle that's weak? We have no idea primary prevention in the rest of these diagnoses. And sudden cardiac death is a major issue in our population.
We personalize ACHD interventions. I mean we are talking about patients that are complex, not any two patients are the same, I'll show examples of that. Here's a patient of mine, a 32-year-old Fontan who had very low oxygen saturations, had a huge network of AVMs. You can see that big gray network of AVMs that made her saturations very, very low.
So with some 4D flow we can see where hepatic venous flow is going. Hepatic venous flow directed towards those AVMs can stop those AVMs, decreases those AVMs, make them go away by redirecting hepatic venous flow. And so by knowing some of this modeling we can then go place a stent, a covered stent, and redirect flow that way. And for this particular patient, her sats went from the mid 60s to the low 80% range, and she's doing much, much better.
With Tetralogy of Fallot, the right ventricular outflow tracks are different for every patient, it's almost like a fingerprint. The surgeons have been in there mucking around and opening it up and cutting, and doing something to that early in life. And so every single outflow track is a little bit different, it's shorter, it's longer, it's wider, they're all different. And so how do we replace a valve in a patient like this besides surgery? Surgeons can go in and certainly put a valve in anything in the right ventricular outflow track.
But I showed you earlier that we're trying to avoid surgery in many patients. So we can take some imaging studies and we can advance that into a modeling. And then we can take that and look at some computation of how that moves. So it's not just the size of it, it's actually how it moves too, is a shortening, is it lengthening? What does it look like when the outflow tract is moving? This makes a difference in terms of trying to predict what kind of valve might fit in there if we're going to try to do something in the Cathlab.
So here's a patient who has a low RVF of 25%, would be a high risk patient. And so we can do some measurements, do some modeling. And we were the first to place this particular valve, first in the world to place this particular valve, which is a Harmony valve. Called the Harmony valve, which you can see is sort of hourglass shape of the valve there in the center.
So to really personalize these types of interventions for patients. You take high risk surgical patients and try to figure out how can we do catheter-based interventions for them. So here is example of a 36-year-old with tetralogy of flow. Four previous open heart surgeries, RVF is very low, obviously 12%, very sick guy. And his course, this is the course going from below, his IVC to his right ventricular outflow track. The surgeon basically put this right ventricular outflow, right ventricular RVP conduit at a horizontal level.
And so nobody could get-- even our best interventionanlist-- could not get a valve out and proper position there. And so we thought of a hybrid way to do this, so doing a subxiphoid incision exposing the right ventricle and then go ahead and getting access there. And then you'll see the valve kind of going in right here. So the valve going in. And so we can place a valve percutaneously and periventricularly. And this particular patient, this was about six years ago, has been doing great since then.
Here's another patient, just thinking about how we have to individualize care. 46-year-old, repaired Tetralogy of Fallot, severe PI, has an ICD. At presentation five years ago, had an LVF of 22%, an RVF of 24%, severe PI and VT. Had an ICD, and was planning, back five years ago, to place a pulmonary valve. We didn't know if it was going to be surgical or how we were going to do it, we were sort of doing the work up. And then he was lost to care, didn't come back.
Just came back about a month or so ago with incessant VT, got controlled with Amio. And was thought he just was not a good surgical candidate. So the question was, can you do a transcatheter pulmonary valve in this high risk guy? EF low on both sides, very, very poor candidate for surgery. So here's his 3D heart model.
See if I can sort of stop this in a certain place.
See a little bit of where his-- He's got RPA stenosis right here. So severe RPA stenosis, and this very abnormal outflow tract where he's got a couple of different areas of narrowing and some wide and large areas. And so we do lots of measurements, lots of measurements through either CT or MRI to try to figure this out. And if you look at valve choices, we have about four valve choices today transcatheter, the Melody valve, the Sapien valve, the Harmony valve, there's two types of Harmony. And then the newer one's Alterra. And Harmony and Alterra are still under a protocol right now.
And so you try to match that up with his outflow track and say hey, can you put a valve in this guy? Because again, high risk, EF's very low. High risk to go the operating room, will any of these valves fit? And our folks felt that there's just no way a valve's going to fit in this guy, just would not fit anatomically into his position. So what can we do?
So we first went and addressed the RPA stenosis, you can see a little bit of it there. His dye pictures aren't as much as others because he also has renal insufficiency. So we placed a stent in the RPA right there. You can see the stent placed to get rid of the RPA stenosis. And then went in, and this is the Melody valve, put a Melody valve in the RPA, in the stent. So this is an injection, right there. And so there's a valve right here, you can see the dye kind of stops right there. Play that again. The dye goes out past the pigtail and then just kind of stops right there because we got rid of the pulmonary efficiency on that side.
Then went to the left primary artery, and this is a Sapien valve right here. And then went ahead and placed a Sapien valve in the LPA right there. And so he's got bilateral-- he's got bilateral valves to relieve his pulmonary insufficiency. And he actually has then no pulmonary insufficiency anymore by having bilateral valves placed. And so that was a unique, very personalized way to approach him that seemed to work.
Here's a 74-year-old with newly diagnosed sinus venosus ASD, anomalous pulmonary vein. And he presented with hypoxia and heart failure and was found to also have liver cirrhosis. So if you look at our guidelines, the ACHA, the [INAUDIBLE] guidelines-- And you pull up what it says about sinus venosus, it says sinus venosus ASD should be fixed surgically. This is not something we typically can do in the Cathlab because the position of the hole and the relationship to the pulmonary vein and the SVC. So this should be surgically fixed.
But this guy had cirrhosis, and Dr. Rajpal said, can we figure out a way to actually do this in the Cathlab? Can we figure out how to do it? And so he put together a 3D heart model, this is the 3D heart model. And I gave it to Saurabh, but he can pass it around if you guys want to see what it looks like. This is his 3D heart model.
You take that 3D heart model and you start figuring out is there a way that we can actually fix this sinus venosus defect in the Cathlab? So basically, can you place a covered stent, something like this, place a covered stent and close off the hole but also not obstruct the vein from behind? The vein, the pulmonary vein, is coming right into that hole, and obviously don't want obstruct the pulmonary vein at the same time. So is there a way to actually do that? And so a 3D heart model is a way to sort of figure that out ahead of time.
So I put an overlay here on the angiogram to kind of orient you a little bit. And so this is obviously the covered stent. The right pulmonary vein is coming right into the SVC, this is the SVC. Here is where the ASD is, it's high, it's up by the SVC. Here's the atrial septum. There's a catheter that's transseptal. So it made a transseptal puncture, it went up into the right upper pulmonary vein to keep that position in place while you go up with the stent. And try to make sure you don't occlude the pulmonary vein when this cover stent goes up.
So here's the angiogram of that. So now the covered stents are already in place. So the hole's completely closed, and we see the catheter up there. And then do an angiogram in the right upper pulmonary vein and it's wide open. So again, if you overextended the stent too much or put it in the wrong position, you would close off that pulmonary vein. And so a non-surgical way, and this is Darren Berman who actually did this procedure, a congenital interventionalist.
We also have to manage complex anatomy and physiology. So a lot of what we do is trying to figure out anatomy. What is the physiology and what can we do to help patients? So here's a 49-year-old with no prior heart disease, presented with chest pain and shortness of breath. So has a very large right ventricle. This is the presentation echocardiogram, right ventricle is huge. Squishing down on the left ventricle, flattening the septum. Obviously concern for volume and pressure.
Here's a four chamber view. This is the right side, left side. And you'll see a bubble study and both sides fill instantly, as soon as the bubbles go in. Should only stay here, fills the left side too. So there's a big defect somewhere. So big right heart, big defect. High pressure in this patient presenting for the first time. And the TR, tricuspid regurgitation, estimated the RV or PA pressure to be quite high, at 85.
Had a TEE that showed another sinus venosus ASD, anomalous pulmonary vein. A cardiac CT confirmed that, and here's the CT. And this is the anomalous vein, coming into, color-coded nicely for all of us. Here's the SVC coming down. Here's the anomalous vein coming right into the SVC, sort of showing that. This particular gentleman's issues were his hemodynamics, and his hemodynamics were awful.
And so let's walk through this. His SVC and IVC flow coming into the right atrium. He's got anomalous pulmonary vein right there. He's got left to right flow across the ASD, and so ultimately, he's got a little bit of a left to right shunt. He's got pulmonary vein sats that are 95, but if you look at his aortic saturation it's 88. And when you do the math for this, he's got a right to left shunt, he's pushing blood right to left across this defect, which is never good. And so his oxygen saturation is decreased systemically.
So you do some calculations, his overall Qp:Qs is 1.3 to 1, but he's going right to left and left or right as well. And why is that? Because his hemodynamics are awful. He's got severely elevated pulmonary pressures, high pressures, mean PA pressure is 53, normal is less than 25. So he's got severe pulmonary hypertension which is left sided. And so we do some calculations, he's got a PVR of 8.3, which is bad. A PVR and SVR ratio, 0.48, anything less than about 0.3 is bad, and he's got high pressures.
But that's not the whole story. The rest of the story is this, he's also got left main stenosis. So here's an angiogram, and there's his left main, is about 80% stenotic right there. You see it in this picture, this is a catheter shooting a left coronary angiogram. And you can see the left main coming off almost like a thread there, right there. It's about 80% stenotic. And why is it stenotic? Because the right pulmonary artery is squishing it. so it's squishing down on the coronary artery.
So if you go to our guidelines, doesn't say anything about this. You go to our guidelines-- and I'm changing Secundum ASD at the top for sinus venosus because they're basically the same concept in terms of considering. And so you pull up the hemodynamic assessment, and he falls under here. His pressures are too high to consider closure. His pressure is too high, his resistance is too high. And so you have to get a consult-- this is what the guidelines say, get a consult with an expert. And we have one.
And so we looked at this patient and we said what do we need to do? Before we can fix the anatomy we've got to fix the physiology. We've got to fix the physiology before we fix the anatomy, that was the key to this particular person. If you go to the operating room and say fix that AD and reroute that vein, and fix that left main, the guy wouldn't survive that surgery, there's no way. Remember how big his heart was, high pressure, high resistance.
So you've got to fix this physiology. And what do you want to fix in this physiology? Well, you want to make his shunt more left to right. You want to get rid of the right to left, if you can do that. And you want to improve his oxygen saturations overall. And you need to change his pressures and resistances over here and here.
So we put him on IV prostacyclin, his story is not done yet, but this is a recent patient. IV prostacyclin, he's better, his saturations are better, he's better. And at some point we going to have to relook at his numbers in the Cathlab and say now is the time to go and do a complete repair. But you have to go full go with him, IV prostacyclin, get his pressures and resistance down, and then we'll fix the anatomy after you fix the physiology.
And this is where the last category is utilizing acquired heart disease for our adult congenital patients. Because there's a wealth of knowledge in acquired heart disease, whether it's in the EP lab, the Cathlab, devices, we need to utilize that to help our patients.
And so here's an example of a 33-year-old with d-transposition, Mustard procedure, had worsening heart failure. An ICD placed in 2014, had high grade heart block and not sustained VT. Here's the high grade heart block, so this is 2014. Here's the VT. So he ends up getting a pacemaker, a dual chamber pacemaker ICD. He's 100 percent V paced, and in 2019 had his first admission for decompensated heart failure.
And if you look at his ejection fractions, this is systemic right ventricle. It wasn't good at the beginning, but now it's worse. If you look at his LVEF, which is the pulmonary ventricle, it normally stays quite well, it's getting worse. And his VO2 in exercise is actually worsened as well. Here's what his 12 lead EKG looks like, it's wide, it's ugly, it's paced.
And so a team of people thought about what can we do, Dr. Bradley again, our pediatric electrophysiologist, one of our congenital heart surgeons, what can we do to help this guy? And so basically a concept is can we do Bi-V pacing? And you can't do Bi-V pacing from the inside of the heart with this, you won't be able to get to the right ventricle from the inside to actually be able to pace. Remember, the other pacemaker lead is in the left ventricle here, so you need to be able to pace here. So you're going to have to do that from the outside of the heart.
There's my little pacemaker, outside of the heart.
And so how we do this is actually pretty unique. Here's a map. And Dr. Hummel is sitting here, so I'm sure I'm not going to say it correctly. But we looked for the last-- we looked for the latest activation. And so this is actually the outside of the heart and this is the inside the heart. And they're trying to match up with the surgeon on the outside, electrophysiologist on the inside, matching up the latest activation point, because you got to know where you want to place this lead. You place it in the wrong place, you won't get effective Bi-V pacing.
And so they found that this was the best place to place the pacemaker lead from the outside. And so the surgeon carved out a little place from the fat right there. And then there it is, and then there comes my cartoon lead being placed on the outside of the heart. And so here's what his heart looked like on chest X-ray beforehand. He's got another stent in his SVC, most of our patients do who have pacemakers. Here's the atrial lead, ventricular lead.
And then here's what he looks like after the epicartial lead. This is the epicartial lead here in place. Here's this EKG beforehand, right here, and then here's his EKG now. And so his QRS has gotten narrow, from 200 milliseconds down to 120. He's also fairly new, about two months in, so hopefully he'll feel better as well. We don't know yet, but we'll see how he does over time. But certainly his EKG looks better.
And then sort of the last is going back to our Fontan patients, the one I've talked about quite a bit. How can we help this patient population? We talked about this elevated pressure in the venous system. All these patients go to Fontan failure, it's inevitable. Every one of them that has Fontan will eventually fail, and we don't have a lot of ways to know how to treat them.
So we began thinking about what can we do to actually treat these patients better? And so we don't know Fontan pressures unless we're in the Cathlab. We have no idea what somebody's Fontan pressures are unless we stick a catheter, you can't estimate it from an echo, there's no way to do that, no non-noninvasive way to do it. So we said, can we use technology that's out there, in this case using technology called CardioMEMS, an intrapulmonary hemodynamic monitor that we can place. So we placed the first ever in a Fontan patient about five or six years ago and reported this particular patient.
Here's actually the PA catheter of this patient. Here's the CardioMEMS recording on the outside of the heart. We've also translated this to other patients, and d-transposition Mustard patients, you can see here. And here's some of the modeling you sometimes do with those devices inside. You kind of see where this might lay when we place it. I'll show you kind of what it looks like when we place it.
We reported our experience. And so here is the CardioMEMS right there on the wire. And then you pop it off of the wire and it kind of sits in the pulmonary artery. This is what it looks like after an angiogram, this is our Fontan patient. And so you can see it's sitting there in the pulmonary artery. And then from the outside of the body you can detect pulmonary pressures, in this case Fontan pressures, it's all connected.
So this is the particular guy. The first guy we did, he had very high Fontan pressures, 32. It took us a year to get him down to 19, but we could only do that because we could frequently check his pressures at home. So at home he lays on a pad, he pushes a button, it sends it directly to us. We know his Fontan pressures every day he decides to send to us. We can make medical adjustments.
We've also been looking at exercise. We can actually find Fontan pressure at exercise as well. We strap on this device with a big ACE wrap on them. We put them on a bike and then the little monitor there, we're actually following their Fontan pressures from the outside while they're exercising, it's pretty remarkable.
So the concept is you have a patient who has in the Cathlab, it's Fontan pressures, in this case, it's about 16, 17, 18 or so, and you want to provide an intervention, whatever that intervention is, to try to see if you can lower pressure. I'll talk about some interventions, but you know how can you then monitor the results of that. So CardioMEMS can do that. So now from the outside of the body we can get a pressure measurement, we can provide another intervention or change our intervention. We can come back and say what does it look like and find out, and then we get another CardioMEMS.
And so the whole concept is that over time, can we have sustained lowering of Fontan pressures, which help end organ disease and help patients along the way. And there have been multiple ideas thought about how can we make Fontan pressures better. Heart failure medicines, maybe, we don't know, we haven't really been able to test that. Diuretics certainly can help. Pulmonary hypertension medicines, there's a lot of interest in pulmonary hypertension medicines with this population, but we have no way of following their pressures without this type of monitoring.
Exercise, yoga's been suggested. Singing has been suggested. Yes, singing. Somebody gave an academic presentation from the Netherlands about singing, and when they had patients who actually were in the choir they had lower Fontan pressures. It's the truth, and it's the Netherlands, so-- Biphasic, this ventilation system has actually been looked at. And then CPAP and BiPAP, we have a lot of interest in that and how that might help patients as well. And then some ideas about leaving a hole. If you leave a pop off for pressure, maybe they'll have lower pressure. Leave a pop off for pressure.
The last concept is that we're trying to get all the adult congenital programs together to have a centralized database, because we really don't have any good prospective data today to look at quality in our patient population. So this is really sort of the future of things.
Curt Daniels, MD, FACC, provides and overview of adult congenital heart disease and details about the Adolescent and Adult Congenital Heart Disease Program at The Ohio State Wexner Medical Center. Dr. Daniels discusses common challenges in ACHD care including, the shifting epidemiology of the CHD population, long term cardiovascular issues for patients with ACHD, caring for the ACHD population and solutions now and in the future.
Related Presenters
Related Videos