Patient was a 78-year-old woman with a prior history of Ebstein’s anomaly, tricuspid valve replacement, diabetes mellitus, paroxysmal atrial fibrillation, complete atrioventricular conduction block and prior dual-chamber pacemaker implantation. In addition, she had chronic blood loss anemia resulting from radiation induced colitis and subsequent bleeding in the colon.
She was placed on apixaban to reduce her risk of cardioembolic stroke resulting from paroxysmal atrial fibrillation. Additionally, she received a blood transfusion for her anemia. Due to her condition and medical history, the Temple Heart & Vascular Institute deemed her a good candidate for the WATCHMAN device to allow for discontinuation of blood thinners in the future.
TEMPLE DIAGNOSTIC FINDINGS
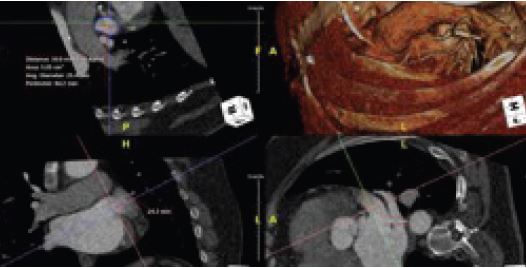
Contrast CT imaging identifying the size and shape of the left atrial appendage in the short axis (top left), horizontal axis (bottom left) and vertical axis (bottom right).

Interoperative transesophageal echocardiogram vistalizing and measuring the left atrial appendage.

Intraoperative transesophageal echocardiogram images of the Watchman device being deployed into the left atrial appendage.
CLINICAL COURSE
- Evaluated by Temple interventional cardiologist
- Determined to be a good candidate for the WATCHMAN device
- Underwent interventional procedure to implant WATCHMAN device
- The WATCHMAN procedure is performed through a small sheath in the groin, without an incision and is completed in most cases in about an hour
- Uncomplicated post-operative course
OUTCOMES
- Was able to stop taking apixaban
- GI bleeding episodes have markedly improved
- Achieved improved quality of life
WHEN TO REFER
Consider referral for the WATCHMAN Implant for patients with a broad range of nonvalvular atrial fibrillation who meet this criteria:
- Have an increased risk for stroke and recommended for anticoagulation (CHA2DS2-VASc
 2 for men, 3 for women)
2 for men, 3 for women) - Have an appropriate reason to seek a non-pharmacological alternative to oral anticoagulants (OACs) such as a history of bleeding complications on blood thinners.
- Be suitable for short-term OAC
KEY POINTS
- Paroxysmal atrial fibrillation is the most common sustained arrhythmia and can lead to the risk of clot formation and subsequent thromboembolic events
- It can affect adults of all ages, but is more common in those over age 65
- Warrants evaluation by heart and vascular experts for diagnosis followed by safe and effective management
- Management includes consideration for medical therapy or the WATCHMAN device
- The WATCHMAN device may be appropriate for any patient taking blood thinners for non-valvular atrial fibrillation
- Any patient on long-term anticoagulant therapy is at increased risk for bleeding complications
- The WATCHMAN device allows for lifelong freedom from blood thinners given to prevent blood clot formation in the heart in patients with atrial fibrillation
- With expert care, paroxysmal atrial fibrillation can be successfully managed
To arrange for a consultation with a Temple specialist at Temple University Hospital or Temple University Hospital – Jeanes Campus, call 800-TEMPLE MED.
All procedures are performed at Temple University Hospital.
Lead Physician
Director, Cardiac Electrophysiology Temple University Hospital – Jeanes Campus

