[MUSIC PLAYING]
EDUARDO ALBENIZ ARBIZU: Here, we have the case of a 70-year-old male patient referred for resection, referred for ESD. Now, you can see how it's the preparation of DiLumen platform. Now, it's very easy just to put some water or saline inside the lumen. And it's very easy to move the endoscope inside the DiLumen.
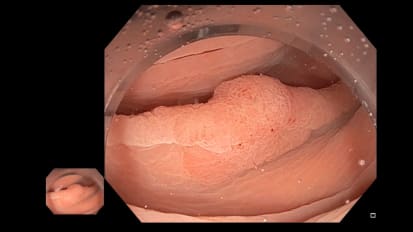
This is a flat lesion in the hepatic flexor. Very difficult to reach, very difficult to maintain the position. It was a lesion at the end with high grade dysplasia.
Now, we are marking. Normally, we don't mark. And here you can see a scar on the lesion. The lesion had a small tattoo and a small scar due to previous manipulation.
In this case, we try to use two balloons, before and after balloon, but we couldn't use it. So we couldn't deploy correctly the before balloon. But the after balloon, it was really helpful for us to maintain a good position, a stable position.
So we mark, we cut. And we decided to perform a standard traction with rubber bands. So here, you can see the before balloon. But we couldn't reach a good position with the two balloons.
Sometimes this happens, but we select this approach with standard rubber bands and clips. So we perform traction. Always we put two or three clips in the band with the lesion. And it was a very difficult ESD due to fat, fibrosis.
So the DiLumen platform helped us to remove the endoscope many times to clean the lens due to the fat. Sometimes we had to cut in blind manner, so we use this kind of knife. We use the knife, dual knife and the IT nano because we had to cut in some blind manner.
Yeah, you can see nice injection, but not in all the parts of the lesion. We are cutting the edge of the lesion so we can remove the endoscope, clean it, insert again. In two minutes, we are in the same position.
So this is a good ability of the platform-- the stabilization, you can remove the endoscope, you can go again with the lesion, with your work. You don't lose the position. Now, it's almost done.
It was a long procedure but the use of DiLumen in this case was critical. Otherwise, probably the ESD could have been a very, very, very long procedure. Now, we are removing the clip that is maintaining the traction.
We can remove the specimen through the DiLumen platform and go in again to see how this cuts. So we are in the right colon. We haven't touched the muscle deeply, but we decided to clip to avoid the later foration or other complications. If we can, we do the closure.
And that's all. We found, in this case, really critical the use of DiLumen. So thank you very much for your attention.