LUO XIAOBEI: Good afternoon, ladies and gentlemen. I am Luo Xiaobei from Nanfang Hospital, Southern Medical University of Guangzhou, China. It's a great honor for me to make this presentation on behalf of Professor Liu Side in the 10th Annual Long Island Live Endoscopy Course.
Today I'm going to show a modified submucosal tunneling endoscopic resection technique, namely double opening STER, or DO-STER, for the removal of large submucosal tumors in the esophagus, as well as gastric fundus near the cardia.
So compared with traditional STER, the key to DO-STER is to deliberately create a second tunnel opening. When the tunnel is extended to the lower edge of the submucosal tumor, a mucosal incision is made to create a second tunnel opening, without the need to continue submucosal tunneling or submucosal dissection on the distal side of the tumor.
So what are the indications for the double opening STER, or DO-STER? Usually we do it for the large submucosal tumors in the esophagus, or the tumors located at the EG junction or gastric fundus near the cardia.
So the second tunnel opening actually enables us to push the submucosal tumor gradually out from the tunnel during the resection, [INAUDIBLE] adequate operative space and improve the visual field, and at the same time it also helps the liquid and blood to flow out from the tunnel easily.
So this was the equipment I used. Usually I use a hybrid knife, or hook knife, and the parameters are as written there.
Next I'm going to show a case of DO-STER. It's a 50-year-old male with no special past history and operation contradictions, and a submucosal tumor was found in the gastric fundus near the cardia. EUS suggested that the tumor was about 4 centimeters in size and originated from the deep layer of the muscularis propria, and was adjacent to a large vessel.
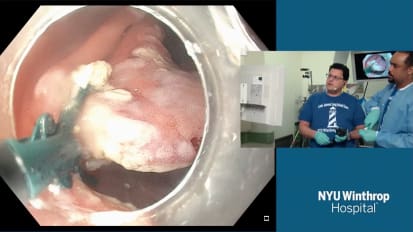
Here is the video of the operation. We can see the large submucosal tumor near the cardia.
So similar to that of traditional STER, our first tunnel opening is made at the lower part of the esophagus, approximately 5 centimeters to the tumor. After that, a submucosal tunnel was created extending to the lower edge of the tumor.
A hook knife, or hybrid knife, is used to create a second tunnel opening in the mucosa over the inferior border of the tumor.
It was not necessary to continue submucosal tunneling or submucosal dissection on the distal side of the tumor. And the length of the second tunnel opening should be dependent on the size of the submucosal tumor, and should be sufficient to allow the tumor to be pushed out through the tunnel opening.
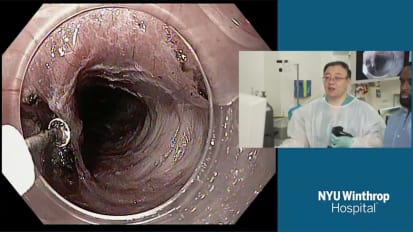
The second tunnel opening also allows the fluid to go out from the tunnel easily.
Now we can see the greater curvature of the gastric body from the tunnel. And this is a second tunnel opening.
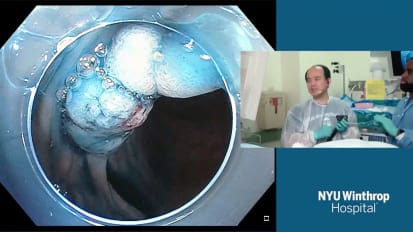
This is a retroflex view of the gastric fundus. We can see the second tunnel opening and the submucosal tumor. When the submucosal tumor was fully exposed, we started to dissect the tumor carefully. If the tumor originates from the deep muscularis, we have to pay more attention.
The tumor was gradually pushed out during the resection, separating the tumor from the muscularis propria. We can see with the second tunnel opening it provides adequate operative space and visual field, and at the same time we can use the tip of the transparent hood to help us to push the tumor out and also help with blunt separation.
When the tumor is fully resected, we can close both tunnel openings with endoclips. This is the second tunnel opening and this was the first one.
This is a specimen of DO-STER. The operating time is about 60 minutes, and en bloc resection was achieved without delayed bleeding or perforation.
This was another procedure. We can see another submucosal tumor in the gastric fundus near the cardia. It measures about 4.5 to 5 centimeters in size, and en bloc resection was also achieved.
So in summary, for such submucosal tumors of the esophagus and EG Junction and submucosal tumors located at difficult operative sites, such as the gastric fundus near the cardia, DO-STER might be a good choice to increase the working space in the tunnel and the reduce the level of difficulty of endoscopic surgery.
Thank you for your time and listening. Now I'm going to move on to the next topic.