Dane J. Genther, MD, FACS is a dual board-certified Facial Plastic and Reconstructive Surgeon and Otolaryngologist (Head and Neck Surgeon) . Dr. Genther specializes exclusively in plastic surgery of the face, head, and neck and performs the full breadth of reconstructive, cosmetic, and functional procedures. Through many years of experience and extensive training, he has gained expertise in the treatment of facial movement disorders (including facial paralysis and synkinesis), skin cancer reconstruction, and revision nasal surgery (rhinoplasty). Additionally, Dr. Genther has advanced training in head and neck microvascular reconstruction. This advanced training in microsurgery allows him to meticulously reconstruct complex defects of the face, head, and neck using free tissue transfer.
Focusing exclusively on facial plastic surgery has allowed Dr. Genther to refine his skills and techniques in order to offer his patients state-of-the-art treatments and optimal surgical outcomes. Board certified in both Facial Plastic and Reconstructive Surgery and Otolaryngology-Head and Neck Surgery, he is among an elite group of only 1,000 surgeons worldwide.
Dr. Genther is an Assistant Professor of Otolaryngology - Head and Neck Surgery at the Cleveland Clinic Lerner College of Medicine and a fellow of the American College of Surgeons. He has published numerous peer-reviewed journal articles on topics such as head and neck cancer reconstruction, treatment of facial paralysis, and rhinoplasty. He has also published multiple book chapters on various topics in facial plastic surgery such as facial reanimation and rhinoplasty. To learn more about dr. Genther, facial paralysis and paresis, and other facial plastic surgery topics, visit Pacific Neruoscience Institute: https://www.pacificneuroscienceinstitute.org
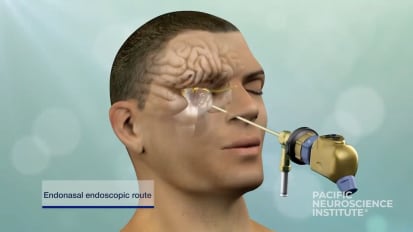
mm hmm, Good afternoon. My name is Amit Kochar. I'd like to thank everyone for attending um one of our pacific neuroscience Institute facial nerve disorder program webinars for the month of june today. We are fortunate to have a friend and colleague who have known for a long time dr dane Ginther who will be talking about smile reanimation and mid facial management and facial paralysis and paralysis. We'll be going through a lot of very complicated surgical procedures that a lot of our patients ask about and are very informed about and so they'll get to see firsthand some of the before and afters and coming from one of the experts in the field. Um like I mentioned, I've known Dr Gunther a long time. We trained at johns Hopkins together after completing his residency at johns Hopkins. Dr Gunther went to Oregon Health and Science University where he completed a fellowship in facial plastic and reconstructive surgery. Arguably one of the best in the country, if not the world. After completing his fellowship, he joined the head neck surgery department, Our center at Cleveland Clinic which is um one of the elite programs in our country for not just training residents and facial plastic surgeons, but also for management of care of patients. Um He works there with two of the giants in our field, Doctor Patrick Byrne and Dr Michael Fritz, who have just made incredible advancements, not just in facial plastics but especially in facial animation. And so we're very lucky to have Dr Gunther speaking today and sharing his experience and so I'm very excited to to hear his talk and we'll be just everyone knows. We'll be recording this. The names of patients or names of participants will all be excluded. But if anyone has any questions, they can please put them into the chat and we'll review them at the end of the session time permitting. Thanks dan. Please please go ahead. Alright, thanks Simon, thanks everybody for joining. Um So I'm gonna be talking about smile reanimation and mid facial management and facial paralysis and paralysis. So it's kind of a broad topic with a variety of treatments, but we'll go through and try to cover as much as we can. Uh some of which is pretty detailed surgical procedures, but also before and afters and concepts about how we planned for these surgeries. No disclosures. So objectives are really to describe the effects of facial paralysis on mid facial cemetery, how those things change over time. And then also in relation to that what what we're trying to treat and what our goals are. Um And then we'll go through these different treatment options and description of techniques and some before and afters to see what kind of effect they can have. So, just briefly, the most common causes of facial paralysis are Bell's palsy and then in our field neo plasm. So, so tumors of the product or acoustic neuroma, vestibular Schwann Omagh's anything that affects the facial nerve and then in terms of recovery, prognosis really depends upon ideology, but also when you start to recover. So the sooner the better if you recover in a couple of weeks, there's a good chance you'll get back to essentially normal. If it takes four or 56 months, there's there's a chance you'll have some synchronicities and some other complications of the healing process. And then we typically say if there's no meaningful recovery by six months, that that usually portends a meaningful, minimal meaningful recovery, in which case the six month point is typically when we consider intervening. So in terms of physical effects, there's kind of two flavors of facial paralysis and paralysis. The first is complete paralysis where its placid sort of a droopy face appearance where there's no movement. The majority of patients are in the other, which is non flaccid or incomplete paralysis. Uh Those patients get a variety of complications, one of which is synchronous, is where essentially the wires get crossed so you get unwanted movements when you smile, your eyes might close your neck tightens up etcetera. Also on the affected side, any any volitional movements trying to smile, close your eyes etcetera tend to be hipaa dynamic and not move as much as they did previously, but at the same time certain muscles of your face and neck will be tight at baseline, causing discomfort in the neck and mid face and all these things together can interfere with speech and eating. And also just a motive display daily, daily display in your life. So the goals of treatment in terms of physically what we're trying to do is really to establish cemetery both at rest and then with movement. So with regard to smile in the mid face specifically. Um Upper lip elevation. Dental show lower lip depression and overall cemetery with the contra lateral or the other side. Um is what we're trying to achieve with these dynamic procedures. And this also has a lot to do with mood, social avoidance, anxiety, personal perception. And these are all things we're trying to create with surgery but also trying to treat the patient and how they feel and um you know how it affects your daily life which can be pretty severe and significant. Um But it's also important to align expectations um to take someone who has a pretty severe paralysis and get back to completely normal is not probably reasonable but to get close or to get drastic. Improvement is very reasonable. So it's important to align goals. Um And then also with a lot of these procedures, additional augmentation procedures or revisions might be needed down the road. So some patients who get a free flap may need a you know a modification of a face lift down the road or eyelid procedures. Uh fillers, Botox, things like that to help really accentuate the symmetry with the contra lateral side. And then in terms of goals of treatment, optimal timing is important too early or too late. And you may burn some bridges or lose some opportunities. So an optimal smile really has 4-5 components. It's oral commissioner excursion. So the lip corner of the mouth moving up. But it's also dental show also lower lip depression which is part of a normal smile. And then that forms the cheek mound which is fullness of your cheeks, demonstrating that you're you're happy and you're smiling. And then the Duchenne smile which is wrinkling around the eyes. That happens when you have an emotive or a truly happy smile differentiates it from just a casual smile walking down the street smiling at a stranger. So in terms of options and algorithm from kind of least invasive to most invasive facial retraining therapy is something that we offer almost all of our patients. Uh We work with several facial physical therapists who are skilled and retraining. Um And we'll go through that in terms of what they can offer. But almost every patient has gotten benefit um whether they get surgery or Botox or not. And then the next thing that we typically do depending on the recovery is key mode innovation or Botox. So selectively weakening certain muscles that so that we can restore symmetry and and stop some unwanted movements. The next in the chain is nerve transfers. So massive the nerve transfer is a common procedure. So it's cross facial nerve graft. These are sometimes used by themselves or in combination with other procedures. Um The next option which I performed less often but certainly is an option for some patients are my enemies or selective muscle excisions and then in that same vein as selective directory which is essentially removing those nerves to the muscles that we don't want to move. The most important that we want to preserve with this procedure and accentuate is any upper lip movement or anything that pulls the lower lip down because those are pretty significant components of a healthy smile. And then temporal is tendon transfer which is moving one of the chewing muscles to the corner of the mouth to give pretty reliable and durable suspension. And also the opportunity for some fairly good movement. And for certain patients that's a that's a great option. And then the kind of the ultimate procedure that we do for any sort of facial paralysis especially complete is that brazil is free flap. So there's multiple ways to do it and there's multiple ways to provide a new nerve input to that muscle. So facial retraining therapy, there's several different options, all of which are achievable and often require daily or weekly or somewhat regular maintenance. Just as you would if you're if you're trying to bodybuilding keep your muscles strong. So one is to maximize the affected side volitional movement. So by isolating certain muscle groups, focusing on contraction and trying to stave off those unwanted movements. You can one try to retrain your brain to move in a way that you wanted to but also you can strengthen those muscles and increase their stamina over time. Additionally you want to decrease the affected side tightness. So hyper tennis city so often this affects the mid face and the neck. So by relaxing these you can allow muscles you want to contract to contract more and be more successful but also it can relieve some discomfort and then didn't decrease in genesis that goes along with kind of focusing on and maximizing your volitional facial movement and what also happens whenever there's any sort of facial weakness. Uh The other side, the non affected side tends to work a little bit too hard and for example the smile pulls a little bit too hard so that accentuates any asymmetry. So getting that to relax and tone down is also an important component. So Botox is the next thing that we typically do and a lot of patients whether they get surgery or not have some sort of protocol where they come in for Botox every 3 to 4 months. So we do this mainly to decrease psychokinesis in any unwanted muscular contraction. So the muscles that we focus on are those that pull down uh the lip so we really want to preserve and accentuate anything that elevates the upper lip um to try and get that to move as much as possible. So it's a bit of a tug of war games. We want the upper lip to win. Um We try to avoid the oral commish er lip elevators and then, or vehicular varies which is the muscle around the mouth. So by affecting that too much you can affect speech. So it's very selective muscle muscle weakness. Uh And then you've got to discuss the goals with the patient, understand that it's a great procedure. It does have a lot of great effects but that it's not perfect and it's not permanent. So one of the most common procedures that we perform is massive nerve transfer where you take the chewing muscle from the large large chewing muscle in your cheek and use that to provide a new signal to your facial muscles or to a new muscle like a godzilla's that you've moved into the face. So we do this with a very small incision um sort of the top half of facelift incisions. So it hides really well. It's just in front of the ear and then in the hairline. So it's often imperceptible once we once we make the incision and close it up and everything heals. So there's multiple different ways to identify the nerve and I'll go through those um In terms of which branch we choose to augment, it depends a little bit on the timing of the procedure. But if someone has functional facial muscles, we want the master nerve too to go to the facial nerve that moves the upper lip the best. So we really want to get the biggest bang for a buck with our signal. And you got to do this typically earlier in the process. So 12 to 18 months after paralysis or in patients with incomplete paralysis and I'll show an example of this. Um even if it's been 10 or 20 years with certain movements of your face, the muscles that we want to contract will it's often with closing your eyes tightly and those muscles will contract. So the muscle works. It's just getting a wrong signal. So we need to upgrade that just kind of the nuts and bolts. So in terms of the sub zygomatic triangle approach to finding the nerve find the zygomatic arch, the post your border of the mandible roughly the course of the frontal branch of the facial nerve. And then essentially by bisecting that triangle will be the master nerve. Another way to do it is identify the root of the zygomatic arch and then three centimeters anterior, one centimeter inferior and about two centimeters deep. To that is where you'll find the nerve. Alternatively, what I tend to do most of the time is you can palpate the sigmoid notch which is uh the gap in the jaw where it attaches uh to the skull where the nerve actually comes out and then runs over into the chewing muscle. There you go. And then once you have that again it's about choosing the right branch. Certain patients or providers prefer to use a branch that has some lower eyelid component. One to support it but also to give more tone to the mid face. The downside of that is that you can get some psychokinesis where you're I might close a little bit too much when you bite down. Um So I tend to use a branch that's almost exclusively upper lip elevators as opposed to including any lower eyelid component. And that seems to work well. And also again you're focusing your your nerve signal on the on the highest value property there and there's the nerve connected. So this is a video of actually a case I did yesterday um for a massive nerve transfer for patients. So we'll go through this now. Narrate. Alright so this is at the beginning of the procedure we have a minimally invasive approach. We're just identifying Arbuckle branch there which will show more there were trying to isolate it and there's three main branches so we stimulate them all. Make sure there's redundancy so that we don't weaken the face too much but also identify a branch that's going to accept the master nerve signal. Um And give a good result. So here we're just dissecting the nerve out as you get into the muscle you want to stimulate and then you can find the muscle contraction. Put the best looper on the nerve to identify it and then we get our nerves set up uh for division and a secure mint. Also we once you find both nerves you can separate some of the massacre muscle which gives you more room to perform your procedure and also have more options in terms of the nerve you select. So there's the massacre nerve, this is our buccal branch that we're going to select one from. Again there's redundancy which is important and then we have our Maciver nerve. So this is the nerve that we're going to use. It stimulates mostly the upper lip elevators with a small I. Component. We cut the nerve and preparation and then now is when we choose and divide formally our buccal branch. So here's the two nerve ends. That's the massacre nerve bundle branch just above it. Then we'll announce the most of those and in about 3-4 months the nerve will regrow and start to give some movement. And then you can see that there's still redundancy with the with the other nerve here. So this is a patient before master nerve transfer who had incomplete paralysis for about 10 years. She came to see me, we did physical therapy and Botox but she was looking for something a little more permanent particularly with her smile. So she was getting a good result with Botox with her neck tightness and I closure. But this was her smile before um expected on the left. You'll see here in a moment. So really no movement there. But also look when she closes her eyes really tightly, those muscles do contract. So it demonstrates that that muscle wants to work. It just is getting the wrong signal. So we actually did a massive nerve transfer to her main buckle on that side as well. And this is her um really about four months post op. So she's still learning how to use it. That's a smile without biting down big smile without biting down and then this is her just learning to use it when she bites down so quite a bit of movement. She didn't really have any on the left prior to this. Okay. All right. And then the next most common nerve graft that we do is cross facial nerve grafting. So we've essentially borrow the signal from the unaffected side. Typically the buccal branch. Again we make sure there's redundancy so they don't weaken the good side of the face. A needing lee. Um If you have functional muscles on the affected side of your face you can directly graft from one nerve to the next. And when it grows in you can get some movement if there's no functional muscles or you have tone and you're looking for more movement. That's where something like a Godzilla's free flap comes in and then across facial nerve graft is a common mechanism to power that flap in terms of which nerves we can use several nerve is most common. But there's various other options from the thought. You can get motor nerve to fastest from the arm. You can get medial ante brachial cutaneous and there's a few others throughout the body that you could use depending on the length that you need. This is just a picture of options for a serial nerve harvest. So the top left is one of the standard stair step approach is so three sometimes four very small incisions are made. The nerve is traced out and then these are closed up in the hell. Well the other is lower left and that's a tendon stripper. So you essentially find the nerve and you can use that tool to kind of follow it up and remove the nerve branches and get the link that you need. And then what's becoming more in vogue these days is endoscopic. So you physically use endoscopes. You can visualize the dissection but with a single small incision. So the motor nerve to bestow this is what we use um sometimes in and of itself but also use it frequently with primary reconstruction after parroted surgery. So the nerve to fastest has a great branching pattern as you can see. So you can actually graph the facial nerve and get pretty good results and lots of different branches. And it's also just underneath the surgical side of how we frequently reconstruct cancer defects. So in terms of how you actually perform the procedure. So it's a minimally invasive approach um on the side that we want to borrow from where we want to find the nerve. It's similar to the master nerve transfer incision in front of the year and into the hairline. And then the green X. There in the middle signals where we're going to find that nerve. And then on the side that we're I'm going to send the nerve to in this case the right side it's just a small incision in front of the ear so that we can see the nerve um and bank it so that we can use it for Godzilla's or a similar approach to on the left. If we're going to use it to to graft directly to a nerve. Just a quick overview of that procedure. So one of the things that can vary from provider to provider is how they harvest the nerve but also how they transfer the nerve across the face. So this is cyril nerve. We did it with stair step incisions and this is actually a Stroker um connected to a plastic drain too. That we used to pass through the face underneath the lip. And it's a small sharp instrument. So it tends to be minimally traumatic when it crosses to the other side of the face. And then you can actually use vacuum assistance and that tube to pull it across to the opposite side. So there you see it and then this is us preparing the nerve um to use the cylinder before the graph. So we're finding a buckle on the good side, there's three branches we found redundancy. So we found the one that that seemed powerful without minimizing input to the good side of the face. And then here's our cross facial nerve graft Nerves are close to each other. Simple anastomosis under the microscope and then give it time to grow in for something like a cross facial nerve graft depending on the length anywhere from 5-9 months. A technique that sometimes used often as a backup as hipaa blossom nerve transfer. So this is often used as a secondary backup to a massacre nerve or cross facial nerve. Often we use to nerve sources whenever doing something like a Godzilla's free flap. One to um provide two different sources of power but also uh some nerves are more reliable than others although they don't have the same desirable characteristics which I'll go through various techniques for transfer depending on the situation with a glass of nerve. So this is a picture from an interesting case and we'll zoom in a bit. This was recently. So this was a patient who previously had a main trunk to hipaa glassell nerve transfer. And we're performing Godzilla's free flap With the cross facial nerve grafts. She had no hips, lateral fifth cranial nerve due to previous radiation and surgery. So we were going to reuse 12 or 11. So here you have cranial nerve. 12 and then there you have the previous nerve graft going into it. So we actually used just after that just distal to it. We did a partial Narada me and use some of those neurons to The primary power source for tone for our flap. And then cross facial nerve graft is the primary source for movement. And then our backup was going to be a cranial nerve 11. The spinal accessory which is rarely used but in her she had very few nerve options. Additional backups again are the spinal accessory you could also do across facial massacre. Um Or a deep temporal selective correct to me is one of the more um it's kind of an up and coming procedure in our field it was kind of recently introduced and becoming more widespread and we're getting more experience with it. Uh it's it's approached with a facelift approach so in front of the ear and out into the hairline. The goal is to identify all nerve branches at the level of the zygomatic archer below. And we want to preserve all branches that elevate the oral commissioner or upper lip and then activate D. L. I. Meaning pulling the lips straight down. So any nerve that dimples the chin pulls the mouth to the side, pulls the mouth down or tightens the neck. Then we want to eliminate those nerves so we transact them and clip them and hopefully they don't regrow which often they don't sometimes there's a little bit of regrowth but we try to take out as much nerve as we can. So it's durable. And then one interesting thing which I found after doing more of these cases typically dl i is thought to come off of marginal mandibular which makes sense because it's immediately adjacent to uh depressed, regulate or s and also mentalities but in several cases it comes off of the cervical branch which also an example of that. Um And it's anatomically it seems a little bit strange but it's also a good thing to know because you could you could uh remove that nerve and not know it and it's important important component of restoring a smile. So this is uh demonstrating mentality contraction in the operating room. So it's important to know which muscles you're contracting and which movement they should have so that you could actually remove the right nerves and be very selective. So this is a patient marginal mandibular nerve with her mentality contracted. Pretty simple. So we know it's contracting. We can remove that nerve and this is a muscle that we want to maintain. This is depressing labia inferiors. So this is pulling the muscle the lower lip straight down, not affecting the oral commissioner but just the lip down. So that's something that's very important. Um And it's often one of the hardest things to restore and facial reanimation surgery. But this procedure has has helped that. And then this is an example of again where the cli branch comes off of the cervical um which again is not described as often happening but I think it's more common than than we think. So I'll show an example of that. So here is you can see Platt is MMA in the neck contracting here and also dl I so the branches are very close to each other. There's there's isolated flat Esma and then D. L. I. And Platt Esma. So this is us stimulating the cervical branch. So play dismal branching, see going to the right and then going deeper as the branch to deal. So again it's it's important to know where these nerves are coming from and also uh where to take them. And this is an example of a patient who came in on the left was her smile prior to and then just two weeks after I was her smile there on the right. So it's greatly improved. She's very happy. Uh There's a little bit of there's more upper lip cemetery. But also you can see that the oral commissioner and the the chin, the lower part of the face isn't pulling as hard so it it smoothes things out and restored symmetry and also she was more comfortable in terms of discomfort after this the next procedure that we frequently do often um in combination with other procedures for various reasons often for cancer reconstruction. But also it's very useful. Um Either in older individuals who have a very kind of topic or droopy lower part of their face. Sicker patients who wouldn't tolerate a larger surgery or patients who would like a pretty durable procedure to restore baseline symmetry at rest in a little bit of movement. So there's various methods to do this um summer through the mouth, only summer through the cheek only. We prefer to do both trans oral and trans facial, since it allows you to really access the important components but also get a good result. So in terms of the technique the temporal tendon attaches to the base of the core, annoyed and the anterior part of the ascending ramus. So we free up that tendon, lift it up to the base of the corridor. I'd use 30. Pds sutures to secure that tendon at the longest component. If you're able to preserve all of it um and get sutures, then you don't need any sort of extension with fashion lotta, which makes the healing process easier, but also more durable. Since you're not, you don't have a connector between your two primary components. It's nice to see the tendon directly into orbit calories. Uh And then I'll go through actually the steps of these procedures. So this is a lady preparing for a temporal standing transfer. You can see on the left, her nasal labial fold is marked. And then on the inside we identify the ascending ramus, make an incision over the ascending ramus. Get down to the bro bone similar to a approach to a fracture. And then there's the glossy component you can see is the temporal, this tendon on the anterior part of the ascending ramus and the base of the core. Annoyed. This is with the tendon freed up to the base of the cord annoyed. So you can see here it's a little bit free and then this is with sutures in it so prior to fully releasing the temporal attendance so that it doesn't pull up and you lose control of it. We get our sutures ready into the longest component. And then we use a uh forceps and then a saw to remove the core annoyed which is where it attaches. It doesn't affect your jaw movement, doesn't really affect chewing, but it allows you to get a really durable tendon that you can then transpose to the corner of the mouth, there's the core annoyed again and then we make a decision in the face. Use blunt dissection to expose particularities. Um If if it's a complete paralysis, there's not much consideration for any muscles attached to that area. But if there is an incomplete paralysis and there is still some tone and movement, we don't want to disturb that. So we can use kind of a blunt instrument and spread in the direction of the muscles and still pass through our our attendant and get a good result and not interrupt that. So we use a penrose drain to pass that through here. You can see it's connecting both both incisions. We passed through our stitches. As you can see here. We also harvest some fashion lotta from the leg because that supports the lower lip. So here we string the fascia lata through the lower lip and out into the midline essentially right through the muscle so that it it uh doesn't bulk up or doesn't move the lip in any strange way. We suture it to the midline of the lip. And then we use that to suspend. Not so much pull but really just suspend and give support to the lower lip in association with our temperatures, tendon transfer. So here are the sutures and the tendons are being sown into the articular varies with the goal of really supporting the upper lip and not just the oral commissioner. And then this is a result right after. Often it looks overcorrected. Uh That's because over time it's going to relax but also um that's just the tension of the muscle as you wake up it tends to be a little bit tense. So this is a guy who had a cancer surgery. So he had a radical prostatectomy. So main trunk of facial nerve was removed. He had nerve grafting intra lateral thigh free flap for contour and then a temporal. This tendon transfer. So this is just two weeks after surgery, his paralysis was on the left with zero facial nerve function. Just temporarily attendance. So if we didn't perform that procedure, you wouldn't expect any movement whatsoever. And then he's actually able to activate it and smile with biting down. Mhm. And then seven months after the same person uh He actually has some of his nerve grafting. Starting to kick in. At this point he had mastered nerve grafting. And also facial nerve grafting. We can see it's a durable result. Still gets good movement, gets a good smile. And then this is an example of another patient. Same thing radical prostatectomy. Radical resection of skin with product A. L. T. But you can see that that it really supports the corner of the mouth as opposed to having a droopy face. Um Which can really affect speaking, swallowing. And also just kind of perception. After recovering from such a big surgery. It's nice to see things as restored as much as possible and to get that support to that side of the face. And then the final procedure that we are the ultimate kind of the the most effective procedure for patients who've had a longstanding paralysis or have an incomplete smile. Um And want want some drastic improvement. Uh The priscilla's free flap is a micro neurovascular. It's a functional muscular unit. So we take nerve vessels and muscle with the goal of having dynamic function in the face to get. It's ideal for anyone with longstanding uh complete paralysis. But it's also useful in some patients with incomplete paralysis with poor upper lip movement and oral excursion. So in terms of design the goal is to have it match as close as possible the opposite side. So all smiles are different. Uh It doesn't matter what kind of smile you have. For the most part it's just that one side looks similar to the other. So some patients don't show any teeth when they smile. Some patients show upper teeth and lower teeth. Some patients have a very muted smile. So it's important to really evaluate the other other side of the face and try to determine exactly what we're shooting for in terms of movement, degree of movement. And that helps us pick our flap and also design how we insert it and how we want it to work and to some degree what power source we choose. So typically for flap innovation. Sometimes single powered meaning just one nerve massive nerve is the most reliable in that fashion. Uh Cross facial nerve grafting can be done as a soul. A soul uh source of innovation but it's not as reliable primarily because it involves too nerve anastomosis and it has a longer course to travel and fewer nerve fibers traveling through it. Just based upon the source nerve. So typically we do either master nerve or two components. So often master nerve and cross face are done together. That's kind of the most common dual innovation. We can do the cross face in that setting one or two stage. The two stage means that we do the cross facial nerve grafting, Give it 6-8 months, let it grow in and then it's ready waiting for us when we do the Priscilla's procedure. The alternative is to do it in one stage where we rely on the massive nerve to really power and support and maintain so that it doesn't atrophy the Godzilla's and then the cross face will grow in later and provide some spontaneous movement. All right, thank you for your attention. Happy to answer any questions. Thanks dan. That was excellent. Um I'm gonna have a couple questions of my own and I'll open it up to the audience. Um Um so I just want to confirm um were you are you doing, are you doing 5/7 and nerve transfers on some of your patients with synchronous is from bells and from like long at like long term psychokinesis. Like what I would call maybe like a partial facial paralysis. I am yes. So not on everyone. So master of transfer works best if you want to add some more strength to the smile and someone who has an incomplete paralysis but not much lip movement, upper lip movement. Some of these patients improved quite a bit with just Botox but some don't. So I typically try Botox for 2 to 3 rounds, see where we can get them kind of find our dose for that patient tae treated as best we can and that if it's still not getting the movement that we want then I offer uh if I think the muscles viable in which case when they close their eyes really tightly and you can see that that muscle pulls that I offer them the procedure since it is pretty minimally invasive. It only takes about an hour and a half and it's just a small incision in front of the year. It's a good it's a good procedure for patients who want movement but don't want a big surgery. Yeah. And then what about when you do selective neural ISIS? Have you ever done a 57 or massive nerve transfer in combination with a selective neural ISIS? Yeah so probably half of the time. So some patients do have decent movement and they respond to certain challenges like lidocaine challenges in the clinic when you can weaken the lower lip muscles. See how much pull you get if they do actually improve quite a bit you can probably get by get by without doing a master nerve transfer. But some patients you just can't get any of that upper lip to move. Unless unless they're really fighting down or or unless they're really closing or closing their eyes tightly. So in that case I would do selective Director Me with Master and Transport. Oh great. Yeah I thought that point you made about the dl I coming off the cervical branch. So just for everybody who who saw who they may have gotten may have gone a little over your heads. The platinum muscle or the muscle in the neck. That causes a lot of that tightness for patients with severe sin kinesis. Um Sometimes in selective neural ISIS will cut that. But you also have to be careful because if you remove, if you're not, if you're not confident that the nerve that's pulling down the lip, which is the movement you want to keep um if you're if you're not careful, you can actually knock both of them out. So it's a really interesting nuance that dr Gunther brought up that I was not aware of. Um There is one question, I have a couple of the but I'll um I'll open it up here. There's a question here where uh panelists asked, is there a bulk with the cross facial nerve graft and massacre nerve transfer without priscilla's? What do you how do you counsel patients on what they'll expect after that? Yeah. So the question was about bulk after. So doing a nerve cross face and Ambassador without doing a Godzilla's graft. Yes. So there's no increase in bulk. So you really have the minimally invasive incisions on both sides right in front of the ear. The master nerve transfer is performed right there. The cross face from the opposite good side to the other. But there's no increased bulk recovery is pretty quick. Um Typically go home the same day. Sometimes you might have a little tiny rubber band drain for a day or so. But otherwise you're back to back to normal business after, you know, a week or so. Um And then the swelling is pretty minimal but can kind of last for a couple of weeks and then go down. Um When we harvest the nerve that's a little bit more noticeable. So we typically use several nerve for the cross facial nerve graft. So that can be a little bit sore and also causes some numbness on the left, around the outside of your foot and lower part of the leg, which most patients get youtube. But it is it is something that you have to consider. Um So some patients select two. Uh do just the 57 um as opposed to adding across facial nerve graft. And um just if you don't mind, would you Kind of go through the how patients are able to make a movement if they were to use instead of the master where they're writing down how would a patient who had a hyper blossom if their master nerve was gone for either from a tumor from other for some other reason they couldn't use it. How would they get movement by using the hyper blossom or the tongue. The nerve for the 12 cranial nerves. Yeah. So it's so it's similar to um massacre and that you're trying to activate the source nerves. So with the five master nerve you bite down because it's normal chewing muscle. Uh Since the hipaa glassell goes to the tongue, most patients um and you can get varying degrees of movement depending on what you do. But a lot of patients push their tongue to the roof of their mouth and that will cause movement. But it also may cause different movement If you move it left, right or down. Or if you can also just tense your tongue. And the reason that happens is the nerve we typically only use about 25-30% of it. So it's impossible to know exactly which nerve, fantastical or is going to which muscle. So you get a little bit of movement and patients tend to figure it out by by kind of trial and error and then and then augmenting uh that with a lot of biofeedback in the mirror and things nice. Um There's another question here for patients with um ocular synchronous or eye closure with bite. Have you done or can you do selective neural license just for the eye or can it be performed for the eye? So you can see that there's been a few studies on this but they've all shown that within one year the orbital symptoms come back. So the reason this happens is one, there's a lot of there's a lot of branching with the facial nerve and there's also just a lot of regrowth nerves are very good at regrowing. Um So they they to some degree will span gaps but also nerve signal from the other side. can also begin to take over as your body recognizes its lost nerve signal. So most people are no longer doing selective your ectomy with an orbital component. If you do it really well, then you typically have trouble closing your eyes for the first few months, then you may get a good outcome for 9 to 12 months and then the symptoms come back. But Botox is very useful with uh ocular symptoms. It's very good at weakening the eye without damaging the ability to close nice. Yeah, I think in my practice, I often tell patients that selective neural ISIS for the eyes, the best way to do it is really Botox is or some type of chemo dean innovation, whether it's Botox or semen or um did support um and uh you know, I think the area that we all really need to focus on and figure out the best avenue for treatment is really that mailer mound, the cheek mound and the cheek elevation. I think the idea that you mentioned assessing if they have functional movement and then trying to figure out how to improve that, like boost it with uh you know, with the nerve to ambassador is great. Um The I've really strongly consider doing that in several patients, but I've never I've done it a few times. I haven't had the best results to be honest. And I think part of it is because I'm not uh focusing on trying to isolate the branch that is not giving an innovation to the to the eye. Or sometimes you get one that has some cross innovation down to the lower lip. So maybe even taking it out even farther in trying to get their super selective in that. Or potentially doing a selective neural ISIS with it at the same time, they actually give you some some benefit. But no, I think this is amazing. I think especially when we're talking about the the now, the different various vectors for uh Priscilla's free flap. Now, obviously that doesn't really qualify for uh adults policy patient or some chinese, this patient. But for those with complete flaccid paralysis, it's really going into the new wave of um innovation to help these patients. There's one question here. Um No, no, that wasn't a question. It was a comment. There's a comment here. Um Oh, actually they're just comments. Um the um the one thing that I, you know, we mentioned last time with dr revenue, and I'd like to get your opinion too. I mean, I think we all go probably the same way, but, you know, there's really no bad time to start getting plugged in with a facial nerve team whether you've had Bell's palsy 10 years ago or 10 months ago, I think um you know, Cleveland clinic where we are here in Los Angeles, as long as you have good physical therapy and doctors that are qualified to do chemo do innovation and offer whatever surgical needs you have um it's never too late to start or to restart if you've taken a break from it. Um Is there any different therapy you offer patients who've been out longer or is it kind of the same, would you kind of start at the same place and have them go through therapy first and then decide what the next steps would be? Yeah, so I agree with with getting connected with, you know, with the facial nerve, facial plastic surgeon as soon as you can. So we actually have a lot of different programs here. We're working with neurosurgery and other, you know, the emergency rooms, things like that to see these patients even before they start to recover. So day one or day 10 and then follow them through the process. So you have all your options. It's time, things kind of evolved. Um but for the patients who are kind of long standing have been dealing with this for a long time, maybe may or may not have been through treatments before, I typically always offer about a month or two. So one or two visits with some home exercises with physical therapy to see where we can get if it's an incomplete paralysis and then we assess where their new baseline is and then start to talk about Botox and other procedures if it's a flaccid paralysis obviously and it's been a long standing and there's no movement, there's only a few options really. Priscilla's and temporal extended transfer in those kind of things. But in a patient with incomplete, I like to assess where we can get with physical therapy so we don't jump in and just start doing you know, even minimally invasive things, but they're still invasive. Um So you know, and then move to Botox. Typically try that once or twice and then we start to see where we can get without surgery and then see where surgery fits into that. And then patients are different to some patients want everything done and want to give it as much as they can. Others want minimal effect on their life and just a bit of improvement in their smile. Some patients are just happy with Botox because it helps them relieve some of their tightness and their ocular symptoms. So it really varies. But I definitely think that starting from the least invasive to kind of more invasive is important. I think that's great. Um There's one last question, I think this will be our last question. This is actually talking about management of belt palsy I believe or Ramsay Hunt. And so how early is it appropriate to treat patients with antivirals? Um Day one a facial paralysis that they're on steroids. Um And so I think you know I'll go ahead and answer this one. Um Typically you know patients want to go to antivirals within the 1st 72 hours um because it would be uh it's used to help prevent the post herpetic neuralgia associated with Bell's palsy or Ramsay Hunt syndrome. Um And if you haven't started within the first three days, I don't think there's any evidence to say it won't help you, but and the the most common uses within that first that first time period. Have you ever given patients antivirals for when you're doing surgery on facial nerve? I mean do you find any reason to do that or have you thought about doing that? No, I never have. Yeah, to be honest I haven't really thought about it but I haven't I haven't seen any. Have you seen any? No it's not no, I haven't seen any patients. I mean even like doing facelifts and other surgeries or prostatectomy is where you're near the nerve. I've never had any reason. So I have not had any patients come back with any breakouts or any any paralysis afterwards. Yeah, but you know, it's interesting question. It's a good question for sure. Um and so we'll we'll leave it at that. Um But dan thank you again for sharing your, these cases, these these amazing procedures that you guys are doing and for educating our audience um for anybody who wasn't able to attend live. We'll be posting this on our end website and our social in the near future. And we'll be linking to dr Gunther as well to the clinic for anyone in the midwest. I would definitely um rather you save your money and travel to see him in Cleveland and come all the way to Los Angeles. Um he's doing some amazing work as or his colleagues and I'm just grateful that you shared your time with us. Thank you so much pain. Thank you. Amit. Mhm, mm hmm. Mhm.