Cerebrovascular neurosurgeon Tomoyoshi Shigematsu, MD, PhD, reviews the evolution of treatment for vein of Galen malformations (VOGM) and then delves into vein of Galen aneurysmal malformations (VGAM) and how they’re classified differently from VOGM. Later, he covers how to treat this particular condition via endovascular techniques.
Chapters (Click to go to chapter start) A typical course for a VGAM and the prevalence of the condition History of VGAM cases and how treatment evolved Cure, in treatment, and death rates for patients treated at Mount Sinai from 2004-2015 Anatomy of a VGAM Symptoms, endovascular treatment, and management of VGAM in neonates, infants, and children Summary and Q&A/discussion
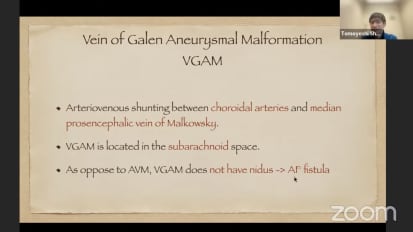
Sorry. It's just takes I guess I'm gonna be there. Yeah. Mhm, mm hmm. Alright, there we go. Mhm. Mhm. So our next speaker is Tomioka Shigematsu and uh como graduated from Osaka University Medical School in Japan. He did his residency at the Japanese Red Cross Society in Wakayama Medical Center um and Osaka University Hospital. He then or doesn't attending um in Osaka University Hospital For multiple years before coming to the United States and working with our team as a neuro endovascular fellow with a pediatric focus with Dr. Bernstein and he's been a clinical instructor and now assistant professor with us since 2018. He's been an exceptional addition to the super vascular team and a mentor for me even when he was a fellow when I wasn't attending um teaching me his skills that he knew and had a varied uh surgical experience from, from what I've learned. And so I really appreciated his uh mentorship and partnership over the years. Um Today it's almost gonna be sharing his experience with the treatment of Janet Yellen, which at this point is one of the most uh experience in the world. So uh thank you tomo stop sharing editor's for kind of interaction. Um mm hmm. Let me start sharing my screen. Ah Is that successful. You see my screen? Perfect. All right, thank you so much. So again thank you for the kind introduction introduction chris um My name is dr I'm on your surgery trained and the vascular surgeon and the cerebral vascular center in Sinai. Um Yeah, so I just wanted to talk about the vein of Galen more information because I'm showing the typical course of the Venezuelan aneurysm. Um more information. Usually the red team residents or the P. R. F. N. P. A. C. Us treating this, this kind of pain of gallant information relatively frequently. Those kids, most of those kids are developing normal stay and picking for two overnight and just just stay at the hotel right and come back in several months. But probably you may not be familiar with this disease is. So I just wanted to present and give some idea what the vein of Galen and there was more more information is and and give you some few points to take home. I would be happy if this helps. You're like residents in the future. They when they, when you guys get the consult about the pentagon's landmark information. If you feel a little bit more comfortable after this presentation, I'll be really happy. Um Let's start with the prevalence is it is said that the pentagon and original mark mentioned it very rare congenital vascular malformation. Listen, 1% of all the ATMs. But recently in Germany nationwide study like 30 billion gallons information born in two years in Germany between 2014 and 2015 which Counts one out of 58,000 still maybe still rare. But if you calculate it in the us it's 62 per year in the US born and born. Um And it is the most common. Several uh driven this amalgamation detective interpreted in Italy and the conflict. 30% of all pediatric vascular malformations kind a lot isn't it? And compared to the other diseases like ah it's let's see like a very famous I'm in acid disorders. It's a lot a lot more than these very famous. I mean that's the disorders. It's very impressive. Yeah. The 1st Venom Gallon Mark Medicine, I don't think it's the true one but it's very famous one. It's dr Jigger uh published a case report with bilateral a trillion is communication to the drain, draining into an originally dilated being a gallon. And this was 19 bodies and subsequently doctor board boundary treated to similar cases and published after these cases. Many authority is the name in vain of gallon. More information of aneurysms for different entities. So it took around 40 years before Dr rebelled found that the ecstatic vein in the vein of gathering more information was in fact the medium bane of the president's different which is the embryonic precursor of the venom gallon itself. So it's not a gallon but it's the precursor of the van of gallon Mark and the shunt is exists right there after this present publish mint doctor loss Jonah's and dr Baron stand. Our dr bernstein established the concept of this thin of gathering more information and described in their textbooks, surgical neuron geographic probably we heard about that textbook and after this uh concept. A lot of reports about the treatment starting come up first Early reports before 2000 generally tends to focus on the technical solutions. So they are introducing that the endovascular surgery may improve these treat improve the outcome of the information. So and probably the surgery surgery is not the way to you years into this baby. Especially in the 80s, they are not able to save this baby but by introducing ah the endovascular Surgery, they're achieving some success. And after 2000 uh much more recent reports focused on more clinical outcomes. Now after getting the strategy of the embolization um the you see that the advancement of the endovascular surgery improved a lot of the prognosis of these patients like around The closest to 80% get the good outcome but still no needs treatment in the new needs maybe a little difficult. Our team reported 80% of total inclusion rate and almost 90% of the good clinical outcome, not the perfect but a good clinical outcome. And this was in 2018 this includes only the patient we started treating in our team so there are more severe cases like coming out coming from the other institute treated previously and they already have some deficits. But applying our strategy, we see a lot of kids start in developing well after ah coming to our facility. Talking about the neon AIDS 10 years ago our team presented the excellent results ah in the management of them units out of, sorry, this is maybe too small. But out of nine cases we only had one death Like and six good outcomes. It's much better than the reports I presented. And I feel slightly before. But I looks into a little bit more recent data and I found that it is still very challenging and difficult. We couldn't save three Babies out of 11. And we had incredibly high complications of hemorrhagic complications. So um and I will talk about the man, neonatal management a little bit later. I like anatomy. So let's talk a little bit about anatomy. I'm going back to this ah picture from raven. So this is um The picture around six between 6 and 11 weeks. And this is that um medium being a person's cephalon which regresses and go away. And this part's going to be the bane of gallons. All right. And this medium bane of President Zeppelin collect the venus a lot from this Alexis. And as you see this vein exists in the subarachnoid space. If you remember about that the IBM, the IBM s usually locates so people star so clearly it's not so broad and so it's a little bit different animal. And so the the vessel supplies the the vein of Galen malformation because of the market mission is here. You can maybe easily understand that these Kuroyedov vessels supplies the bane of the landmark mission. This is the scheme showing the vein of Galen malformation. Looking from the side. This is the internal karate, this is a battler. So nice. Number five is the entire corridor artery and this is the number four. This is the serial corridor artery coming off from these corridor arteries and the supplies. And the one coming from the top which is the posterior colossal artery. It's a branch at the end of the until three a. c. a. This goes through the vein of yelling. So the coronal arteries supply the venom gallant. And I told you this is the subarachnoid space. And so which subarachnoid spaces here? This reactionary spaces here gallon usually exists here. The blue circle. Maybe this is a big element er positive system. And the green circle here is the graduate germinal system. So now you have time there. I think you have an image where the venue Gallimard information exists. And one more thing I had to let you know is the venom gel in. Um Our information is considered as a Chilean official, it's not a more information. So it doesn't have an itis. So the artery directly connected to the vein and there are some small vessels around it. But those are the angiogenesis I think and the targets. So the targets of the treatment itself. We have to close the fish or the bank. So it's very similar concept to draw the efforts Stock economy recently reviewed in the grand rounds, right? And I will go to the classification of the information next. Mhm. You know, if you open Microsoft neurosurgery by Dr Acevedo, you'll see his classification based on the surgical anatomy. I found out recently that I found it it's very interesting. But because it's a surgical is not a good option at this moment. Uh I'm not gonna talk about this But from the neurovascular standpoint Dr. Watson is classified into two types as this is not a Kuroda type and be in europe mural type. Right. So we go back to this picture again, the median being a president cephalon regress from the front. So it goes away. And then only this much remains. If the fish happens in this place it's Carrillo and then later if the fisher happens here and back, it's mural, it's kind of, that's where I, I understand the corridor type of the aneurysm malformation has multiple high flow officials in this network here and it exists a little bit more until really like deep in the development deposit them or the corridor fishers. And the mural type has a few fish. There are not many directly to this ball and locate a little bit more seriously maybe credit criminal sister. And you have to think separately about from this then of gallons are under original dietitian, which is like a somewhere like Salaam IQ or anywhere in the N. B. A. B. Mark from IBM drains into the ah being a gallon and then subsequently the Venezuelan enlarged. So this is totally a different animal. Ah Mhm. You have to think separate. This is example corridor type and you're a type. You see a lot of big vessels getting into the more information fish creating the official here directly. And even from the A. C. A. It's a little bit located materially, whereas the mural type has a few fish too well and just go directly to the, almost directly to the ball. Dilated part, all the symptoms. I made it very simple. This is this is not, I don't know, this is not explaining everything. But I made it very simple. New mates present with congestive heart failure and most of them are corridor type in front afterwards they present with hydrocephalus microcephaly. And most of them are mural type of course. After trading the corridor type, they can developed hydrocephalus lately, even if they're a prototype. But I made it very simple. It's very, I think this way it's very easy to understand and the other symptoms like development is the way our seizures. Derek described, love, love, love. So based on these knowledge what kind of treatment as the top before. Ah And the vascular treatment is going to be the main part of course. But the strategy is staged trans arterial embolization. So within a certain limit of radiation contrast to it per one session. We tried to close the fissure, not the feeders, fish like sell as many as possible enough so that we can reduce the flow. And so that we can allow the baby to grow normally. Okay, So we don't want to take too much risk. We don't want to make it worse. So if the access in getting into these small vessels seems to be very difficult. We just stopped that session and then let the vessel grow or let the vessel go away myself. Or if the patient is very symptomatic, we have to take a risk and get into a smaller vessel and close more vessel more official. But this is the treatment there. We need to know other management as well about the mom. The baby is still in the belly. So we can manage a little bit During the babies in the belly. His mom's belly. Um around I think around 20 weeks. The then on the other. My information is detectable in fetal ultrasound. Yeah, but it on the left of only if the procedure is. Think about it. It's detective over the color Doppler. And after the diagnosis or the detection of screening under the federal M. R. I. Shows a very beautiful pictures which was diagnosed then a gallon. More information like this. And we also can see the brain itself. We sometimes see significant brain damage already. And we had some ah in those cases. Unfortunately we couldn't offer any treatment. And also the ultrasound is very useful as to assess the cardiac function. And if the baby already had the cardiac heart failure we may give the jagat Singh to the mom. Okay. And there is no evidence yet which if the C. Section or is better the general but their labor is also what you find but to manage the timing because we have to get ready. I'm going to talk about that and then the only next but you have to get ready to manage the timing. C. Section is preferred but it's not necessary. So as I told you we have to get ready when the baby comes out and it's going to be the bit huge teamwork including your B. C. O. N. And nick you piece cardiologists, peace and your surgery of course pediatrician, neural radiologists and anesthesiologists and our near IR as us you have to get together and then discuss and evaluate the immediate uh the baby needs to be evaluated immediately. Maybe the baby needs intubation I don't think. But really we really need to ask them to get the umbilical access that's very crucial for the treatment or to get ready for the treatment. Okay? There are two us with galleries and then to you one and we also asked to go we have to get a call and M. R. I. To decide the indication of endovascular treatment. If everything is good, the baby doesn't need to get undergo the endovascular treatment. But if the baby has a good brain and if we see the apostolic reverse flow and distal arctic art in the echo we don't wait we go for the endovascular surgery because we know that if the baby has this diastolic rivers flow in this arctic arch the baby is going to get worse for sure. And since we have in the vascular surgery established we don't wait. This is how we get we go into the vascular system. Usually we use the trans umbilical access and like this and with the transcultural NBC embolization and repeat the embolization until the baby gets out of heart failure. Sometimes it takes like 34 times for four and a vascular surgery sessions. It is almost impossible to close whole fish live in one session and it's very also dangerous. We don't want to close everything at once. Me because the frog because of the fragile premature journal layer or the profusion pressure breaks there accused of several edema or bleeding like subarachnoid hemorrhage, economic or other. I ch you know what happened if he closed too much. So it's a very sensitive balance of the risk and effectiveness right? Um Just quickly go review we go very very close or past official fast fish like self and then close the official. That's our strategy and this is the glue injection video. Yeah close the fish like this. Um Sometimes we find we see other teams using coils and onyx. Right close the fish love with coil and then inject the symbolic material. Close the fish again like like this. And then and they used the anabolic material just to close the theaters. It's very effective. It is very effective to reduce the flow in the vein of Gallimore information of course. And that takes the baby out of the heart failure but insufficient inclusion of official. It doesn't quote official itself. It recruits small vessels in the future slowly and in genesis. This makes the further treatment in their later age very difficult and higher risk. So this is one of the you know that we do not use coils. We think the coils blocked the hope well once the baby gets out of the heart heart failure we let the baby grow and next is the management of the infant. So and during the infancy we set up a pediatrician or pediatric neurologist. Follow up to monitor crawling clinically to make sure that baby needs the milestones. Okay. And we also get the head C. T. 124 and six months to monitor hydrocephalus or consultation or any features of melting brain syndrome. We usually have a kid grow Like 5 8 months before starting the endovascular treatment staged if it's the babies cardiac condition gets worse. It's not stable or we see any hydrocephalus or anything like that or regression delay of milestones. Those things you can ah A lot of us and then we sometimes do that earlier in the last year intervention of course. And um we see if the patient doesn't gain weight. Doesn't drink doesn't not well doesn't eat. Well that means that it's called failure to thrive. That's the way how we know that the patient cardiac condition is not there. But let's talk about the hydrocephalus a little bit. So it happens anytime even in the fetus or neonics it happens but most more frequent and intense but instead of actual obstruction of the aqueduct from the vein of dilated vein of yelling this it is said that the venus hypertension is the cause of the hydro surface. Not so it's usually it's not obstructive hydrocephalus so that the CSF does not get absorbed properly. So urgent embolization Should be carried out 1st. Not a very efficient. The baby may need to be patient later but not to begin with. There is a very high hemorrhagic complication risk. It's 40 like close to 50% in our cohort. And recently endoscopic E. T. V. Is also an alternative a good alternative that we've been doing recently that we got done having a good results Euron present in your case with obvious hydra sessions. As you see. Yeah we um we um we did just normalization. No chance being together and start drinking nos then keep symbolizing and then the venture, the size of the venture can normalize and the venue yelling get cured. This is how we treat the mentioned even if the patients present with hydrocephalus. So um I'll just summarize so they've been on gallium arsenide itself actually the venom Gallimore information is not the official right? The correct name is the venom gallon. Unreasonable, more information. Right? So it is a gov and especially in the media ban of the president's shuffling, it has a corridor type and neural type. And now the strategy is stage translates to you're an older version to make the baby grow normally and targeting the official, not not just the artery targeting the fish. And the treatment is very crucial. And even if you see the hydro syphilis that needs to be managed with embolization first, still about the venerable Martians, there's a lot of place to improve and like for instance, if we need to save more babies units and there may be a different strategy, trans venus symbol. Ization. Maybe there's a genetic thing and there is a place that interview during prenatal intervention, there'll be, there'll be your place. So if you're interested in if you become interested or if you're interested in this ah field, Feel free to reach out to Dr. 50 is a pediatric directors here for me of course, ah and we can work together to make these to save these babies. Okay, thank you. Are there any questions? Yeah. Um, I can ask a question. Thanks a lot for that. Very helpful. And even having gone a couple of beers during fellowship still really appreciate the detail that you can provide. Um But my question is in the past, in your experience over your past your career so far, what has been the biggest innovation in treatment of the biggest kind of paradigm shift um in the in the past 20 years or so. Do you think about the treatment of the van? And we got it right. Yeah. Well of course the that's it. The introduction of the endovascular surgery is to this baby and and availability to apply this in the vascular surgery to this tiny tiny baby is the big uh success to treat this space to these kinds of patients to do that. It's not just the entire basket surgery. It's just Nikki management and west asia management and and also at the same time it's more well understood that this disease is more well understood understood at this moment. Okay, how about umbilical artery, how big an impact has that had umbilical artery? How about umbilical artery access? That Alex is so fond of. Mm hmm. Yes. So we know that this under now we understand this disease. We know that we this baby needs uh uh stabilization. So umbilical artery access really helps ah not just management in the new needs but it helps the other the later treatment to get to give us an access. Then we really need this umbilical access ah at at the beginning. So we have to obtain the access of the Kalahari access. It's a very very huge impact in treating. And that's relatively recent, isn't it? At least making it routine Joanna is isn't that you didn't start out doing that did you? It was um It came about but it was probably uh more than um 15 years ago where it became routine. Um But yeah if you when we receive patients for instance transferred or uh for whatever reason we can't get umbilical artery access in the neonatal. Then there's a very high percentage of patients that go on to include the femoral artery which isn't necessarily, most of the time is not problematic for limb development but they develop small collaterals but it becomes problematic for repeat embolization. So later on it makes access very difficult um if they require repeat hospitalizations. So yeah it's been a it's been very useful. We we pushed them especially when they're born here. They're used to the Nicu here is very used to getting those access the access for us. Yes, Dr. Bernstein reported in 1998 the first time. And yes in the first report with the neonics we we presented in 2010 was most of them was transformer surprisingly actually, but now we really no that transcend Jericho is necessary for management of these patients and it's making better outcome, Joanna. Did you have any other comments on this otherwise beautiful presentation. No it was it was a great presentation. Um I think I think it's it's true and we I can't emphasize this is one way um that dr Berenstein and our group of developed and treating other other places don't have the expertise or think other, you know, other methods are better, such as trans venous. I don't think Toma mentioned this, but we we've seen that those other methods have higher complication rates, so hemorrhage in the neonatal and that sort of thing. So, um, you know, I think even though this is sort of a more fastidious method, it might require multiple treatments. It our clinical outcomes are uh speak for themselves. It's it's uh in our opinion, the best way to do it. Mhm. That's great, mm hmm. Another world class program at Sinai. Mhm. That's great. Okay, we've reached 9:00 that concludes our grand rounds for today. Have a great day.
Related Presenters