Chapters
Transcript
[MUSIC PLAYING]
MACEY NELSON: Thank you, everyone, for joining tonight's discussion, Sharing Perspectives on the Reconstructive Lumpectomy, a discussion for surgeons and radiation oncologists. My name is Macey Nelson, Senior Manager, Medical Education for Breast Surgery.
And I'm going to be one of your co-hosts for tonight. I'm excited to be here, but, more importantly, I'm excited to be joined by four of my colleagues for an insightful discussion. My other co-host this evening is Dr. Anthony Lucci, from M.D. Anderson Department of Breast Surgical Oncology, University of Texas, Dr. Karen Barbosa, University of Maryland Shore Regional Health, and two radiation oncologists, Dr. Asal Rahimi, an Associate Professor of Radiation Oncology with UT Southwestern Medical Center, and finally Joshua Mondschein, Tennessee Oncology Provision Proton Therapy Center.
We are hopeful that tonight's session is going to spark meaningful conversation and discussion on technology's impact on the surgeon and the radiation oncology partnership. But before we get started, I want to walk you through a couple of housekeeping items. First and foremost, we're going to start tonight's session with a brief BioZorb overview led by Dr. Barbosa.
And then we're going to segue into a roundtable discussion. And this truly will be a roundtable discussion. So we encourage you all throughout the night, if you have a question, please do drop it into the question section of your screen, and we will do our absolute best to bring your comment, rather your question, into the conversation
Following tonight's session, there is going to be a survey that we're going to send you. And the surveys are incredibly valuable. And, in fact, the survey from our last webinar back in May was some of the information that we used for the topics tonight. So if you were at that session in May, this event will feel somewhat similar. On the screen you should be seeing some polling questions. If you haven't had a chance to answer those poll questions, please do, because that also gives us really important information, so our faculty can adjust and tailor some of their answers based upon our audience members tonight.
I'm going to give you just one more quick moment to take the poll. Our panelists are experienced clinicians, and they are here to discuss complex issues and challenges, along with potential solutions that surgeons and radiation oncologists are encountering as they aim to treat patients with breast cancer. So Dr. Barbosa, please do introduce us to BioZorb.
KAREN BARBOSA: OK. Thank you for having me. I want to thank Hologic for having this webinar. I think it's really helpful, especially in the time of COVID, to be able to see someone and interact and get an education.
One of the things that I'd like to do is just briefly touch on some of our disclosures that the panelists have. So we'll get that out of the way. The disclosure I have is $200 worth of Genomic Health stock, that I bought as a fellow, Lumicell, I'm a consultant for one of their research projects. I am a consultant for Hologic, as are the other panelists tonight. I am also a consultant for Stryker, data research. And Dr. Asal has her disclosure here for her grant for Accuray and educational speaker.
All right, now that we've got the housekeeping out of the way, let's do an aerial view of what BioZorb is. So basically it's a 3D marker that we use to place in the tumor bed to mark the tumor cavity. It's bio-absorbable, it has titanium clips that are embedded in it so they don't move. It's built into this lattice that is a framework. The bio-absorbable framework will slowly incorporate over time.
And incorporation time really varies depending on the patient's breast tissue, I found. When I first started working with BioZorb, they said it was about two years. I've had patients that say they can kind of feel it at three years, and by four years it's less palpable, and by five years they don't feel it. So it's variable. And I've had patients that in the first year they don't feel it at all. So some of it it'll be the patient's body habitus and their breast tissue. Part of it will also be the type of BioZorb and the location you use it in.
So that's going to be all of what we discuss tonight, a little bit later on. But it's very important to understand that the discussion should be had regarding the fact that it does get incorporated into the breast tissue and can be palpable. Like I said, this is valuable because it marks the tumor bed cavity. And it helps us as surgeons recreate the breast form. I use it as scaffolding.
So when we look at the different types, you can see here on this slide that we have several different sizes, but the different designs as well. The spiral is more full and gives you more volume. And that is best placed in the lower outer or inner quadrant or the upper outer quadrant where you have a lot more breast tissue. The low profile is really great for the upper inner quadrant, where we don't have a lot of breast tissue medially, and we're going to try to bring breast tissue to cover it, and you don't have a lot of wiggle room.
The more volume of tissue that you have to place over the BioZorb, the less palpable it's going to be to the patient, and the more it's going to be able to recreate the form. So having a variety of different sizes is really helpful, as well as the different shapes. And what we hope to do is try to incorporate this into today's teaching, for how to use each and where. This picture, I think, is really great because it shows you that on the first slide the BioZorb here is really incorporated into the breast tissue.
And I can speak to this myself. This isn't my slide, but what I will tell you is that I actually had a patient who didn't follow up on her treatment and then eventually needed a mastectomy. And when we sliced the specimen, pathology showed the same incorporation, which was pretty incredible, to see how well, and I think, in hers was only two years afterwards, that we found such a great incorporation. And you can see the pathology in the middle there, and at the end you can see how it looks before it's really gotten incorporated, if you take it out sooner.
I'm going to go to the next slide. The next slide here is a great example of why it's so beneficial for the radiologist to see. A lot of times we'll place clips, and clips can migrate. But the BioZorb will stay in the tumor bed nicely, while it creates scaffolding for the reconstruction. But you can also see beautifully how it delineates the cavity bed, so the radiologist, for years to come, can look at this and re-evaluate whether there is calcifications that are nearby the tumor bed or some tissue that feels abnormal.
So it's really nice, and patients like to see this as well, because they can see it very distinctly on their imaging. The other thing that's important is here, when we look at it, it's very easy to see on imaging the 3D marker, and we can see this-- once again this isn't my slide-- but you can see the 3D marker after chemotherapy here. And if we go to the next slide, this is what we used to have back in the day prior to the BioZorb. We would mark it with clips that could migrate.
And even before that, before clips, there were some surgeons that just literally would move tissue, and there'd be these seroma cavities that would be left in the deficit, where that would be the target planning for the radiation oncologist. So I think that when you see the difference of how well the BioZorb, from this previous slide to this slide, you know it really limits the amount of radiation that you're going to be exposing a patient to, because seromas can track under the tissue planes, even if you're not moving flaps. And when we look at oncoplasty, we're removing a lot of tissue. You create a lot more tracking of seromas if you have any.
So I'll go to the next slide here. And this is a CT axial guide. For those of you who aren't familiar, the pictures are a little bit small, but this is a great delineation between where we were with clips and a seroma, to where we are now with BioZorb clearly marking the tumor bed and really giving us a precise tumor marker and target. So if we continue on, and we look at why are we doing this.
Here is breast tissue conservation challenges, right? Patients want to keep their breast. They want to have sensation. They don't want to overdo their surgery, and especially in the day and age of COVID, some of them are just afraid to go to the OR, so being in the hospital for a long period of time, or having the risk of a complication or an infection is a concern. When we look at these you're looking at deformities that are caused by volume loss. And these are most likely closed with the fact that there is a seroma there that eventually will get incorporated or absorbed over time and/or get incorporated or absorbed and radiated at the same time.
And that'll only exacerbate the dimpling. So when we look at the last one, this is what's called a bird beak deformity. So if you look on your screen, that inferior pole, if you take out that tissue, it looks great. And surgeons will be very proud of themselves in the post-op period, because the seroma fills it up beautifully. But over time that fluid will get incorporated and absorbed even if you don't do radiation.
But if you add radiation to that, it's only going to make the breast tissue more fibrotic. It's going to scar it down. And then you're going to get this bird beak deformity that's really difficult to treat. So oncoplastic surgery gives you techniques that you can use in the lower pole of the breast to reapproximate breast tissue, BioZorb creating some volume, so you can recreate the form. The two of these blend perfectly.
And then we don't have to pick on our surgical beds as they get radiated, and we don't have to pick on our radiation oncology colleagues for damaging our work. Actually, the onus is on the breast surgeon to tee it up for the rad-onc, so that they don't have to worry they can do their job, if we do our job a little bit better. And that's where oncoplasty really rolls in and does a great job of helping the rad-oncs get a good outcome cosmetically, if we set them up for success.
So in this slide, this is kind of a blending of the technology of surgical oncoplasty fused with the BioZorb that clearly marks the tumor bed cavity. And, like I mentioned, I use it as a scaffolding where I can rotate flaps of tissue over the cavity and obliterate the BioZorb so that it's not exposed. You never want that, but that you can get these great forms where, to a lot of people, they don't even realize they've had surgery. The scars will fade, and you can get a really nice cosmetic outcome.
So when we start looking at doing oncoplastic surgery, some of the things that we want to suggest, you know, tips for oncoplasty 101 and how to work with that. The most important thing is kind of what we're doing here tonight, which is getting all of your colleagues on board. I had places that were calling my post-surgical cavities with BioZorb a BI-RADS 3. There's a mass there. They didn't understand that that clip, and what they were seeing, was a BioZorb.
So making sure your radiologists know what it is, making sure your rad-oncs know that you've placed one, because when you're placing them, you might be rotating large flaps of tissue. And it might not represent where the surgical scar is. Making sure that, if you're not adept at doing some of the larger excisions and reconstructions by yourself, that you're comfortable working with your plastic surgeon.
You can work together. And that's basically going to be what your comfort level is, what your plastic surgeon's comfort level is. But I think that the camaraderie, working with your plastic surgeon and you, especially if you're new to this, can be the most beneficial teamwork available. And like I said, the medical oncologists like to know, because sometimes if they are doing an exam, it's helpful for them to understand that you've done the surgery and how you've reconstructed the patient, just so that they understand, maybe there is something that's a little palpable in the post-op, but that'll soften over time.
Mammo techs want to be aware of it. And you also want to make sure that you dictated in your op notes, so that you can refer back in years to come and say, wow, this patient looks great. Did I use the BioZorb on this, or was this before I started using BioZorb? It's nice to have that comparison that you can go back in your notes and look at who you used, what and what size. And it's a learning curve as you progress through using these technologies, whether it's just the surgical skills and/or in conjunction with a BioZorb marker.
And then also let the PCP know. Let them, the primary care doctors, they're going to be feeling these patients and looking at them. So letting them know what you've done, I think it's pretty helpful. So let's go to the next slide here. Setting expectations, I think this is a really important slide to discuss, because when we look at expectations, it's not just expectations of you and what you're hoping to provide to the patient with a good cosmetic outcome, but, more importantly, the expectations of the patient, letting them know that they are going to be having their cancer removed, that positive margins are still possible.
Even though you're taking out this cancer and using surgical oncology techniques that optimize the cosmetics, this is still cancer surgery. What I always explain is you can't see it, you can't feel it. Even with palpable masses, at best, you're getting a guesstimation of the true side. There might be some microscopic disease that will be evaluated further on the surgical pathology.
So basically what I do, is set the patient up to understand what we're looking at and what we're trying to achieve, pre-op education, once again. What we're trying to do is basically take out the cancer, try to take out more tissue with a negative margin to avoid a take-back, and at the same time be able to recreate the breast form, so that they're left with a scar, which we can't help but leave them with a scar, but hiding the scar. Periareolar inframammary fold, axillary, we're really trying to move away from making large incisions on the belly of the breast or around the breast that are visible.
And when we have these abilities to make these incisions, it helps patients psychologically. They're not looking in the mirror all the time and seeing a scar right in their cleavage, when they were having a low-cut dress, or at the beach in a bikini. And like I said several times, the palpability, and I'll stress it again. Palpability is best addressed pre-operatively, up front, when you introduce the option of bringing it into their surgery.
I also put it on my consent. When we look at the palpability, like I said, I've seen patients who have a relatively prominent profile spiral, and yet they don't feel it in the upper inner quadrant, because they have so much breast tissue. Or they have an older patient with more glandular tissue, where I like to actually get a little bit more coverage. I believe the Hologic perspective is 2 centimeters above is fine. But I always say, if you've got glandular, older breast tissue, you want to be careful because glandular, older breast tissue has a higher propensity towards fat necrosis.
So, once again, it's the size, it's the type that you're using, the shape, whether it's a spiral or a low profile. And where do you put it? And I've heard a lot of people say, rub it like you love it. And rubbing the site really won't affect the absorption rate. But I think some patients like to feel like they're doing something, so that I'll leave that up to the surgeon's discretion.
When we look at surgical techniques and abilities, basically marking the tumor bed, talking about who's a candidate for radiation and knowing if you're going to radiate something, giving them a little bit more wiggle room. If you're planning to do catheter, APBI, patient education, like I said, I put it on my consent form. Contraindication, if there's an active site of infection, you really don't want to be putting that in there. Because just like any other implant, you don't put implants in a bed of infection
I always use IV antibiotics pre-operatively. I always try to orient my BioZorb and suture it in. And we'll talk a little bit more about that later. And it goes back to size, selection, and location. And it doesn't always need to be the same size as the tumor. That was, I think, initial training. But now what we're really trying to do is reapproximate the breast tissue around the BioZorb. So once the cancer is out, even if it's this, we're bringing the edges together. And we're really closing down circumferentially around the tumor.
And that's why the importance of the BioZorb is really there, so we can radiate less tissue, but really get the margins that were around your initial cancer. So full coverage, single insertion brachy catheter might be difficult. But I've heard of some people trying to do that. Location and fat composition of the breast is really going to be what your overriding guiding factor is, as to what to use and when and where.
When you have really large breasts, you really want to avoid that thin skin flap for anterior coverage. And, like I said, the glandular older breast tissue is going to be more at risk. If you have a young, dense-breasted woman, then you're going to be able to get away with a little bit less tissue. But, like I said, 2 centimeters at least of coverage is always a good idea, because if you place it too superficial you can cause some sucking in. And you don't want that. You really don't want to set up your rad-oncs for failure.
Like I said, it's really in the hands of the surgeon. So let's just take a quick look at this. When we talk about oncoplasty, you can see, just looking at this slide, there's a variety of approaches. And where we make our scar doesn't always represent where we're actually taking the cancer out, because you can see we can get almost to any quadrant depending on our surgical approach.
JOSHUA MONDSCHEIN: Yeah, Karen, this is a really interesting slide, and really important for a radiation oncologist to see. When patients come in and see us in consultation, the next step is for them to have a planning scan or a CT scan to let us plan the radiation. And at that time we really outline all of the breast tissue. But we also outline the scar, which, to us, typically represents where the tumor was removed.
So in cases of oncoplastic surgery, where you're obliterating the cavity, so you don't have a seroma to target, and oftentimes clips may not be left behind, if you don't have a BioZorb device, then you're really left, as a radiation oncologist, guessing where that tumor was located, because you really don't have any of the three, the scar to help you, or the seroma or clips. So that kind of brings up a unique challenge for radiation oncologists.
KAREN BARBOSA: Yeah.
ANTHONY LUCCI: So, Karen, I thought that was a really great overview on the BioZorb. And I think, obviously, nowadays we as surgeons have the ability to move tissue around and to do oncoplastic reconstruction, which I know you're going to talk about more in detail. But I want to stop for a minute and ask our radiation oncology colleagues, when we move the tissue, what can we be doing as surgeons to make this easier for you to know exactly where you want to target, how you do your planning?
I'll start with Dr. Rahimi. What do you think, I know many of us for years have used clips. We just put clips around each of the margins. Is that adequate? Or do you really prefer something like BioZorb?
ASAL RAHIMI: So, I mean, any kind of marking is really great. The issue, though, is that now that we're getting into this era of more oncoplastics, with just clips, the clips can be all over the breast, just depending on what type of manipulation has been done with the oncoplastic surgery. So what we're seeing is that a lot of patients want to come in in their early stage, and they're candidates for partial breast, but they're not eligible anymore for partial breast, just because the clips are all over the place, or there are no clips.
So this has become a really big challenge in the era of partial breast irradiation, and especially now, with all the new data that has come out, that has shown that whole breast radiation or partial breast is equivalent to whole breast radiation. People want partial breast irradiation.
And they can't have it sometimes in situations when we don't have that communication between the radiation oncologist and the surgeon. So having a device in there that localizes exactly where the clips are, before a lot of that manipulation happens, is very crucial to being able to do partial breast irradiation in the era of oncoplastic surgery.
And I think just having the team working together, and discussing these issues and really knowing what job each one of us has to do and how we can make it better for the patient, is really crucial to make that happen, to make that successful.
ANTHONY LUCCI: Yeah, that's really good. Dr. Mondschein, what about you. Do you have some thoughts to help? Because I think the whole point of this is to facilitate a discussion of what we can be doing as surgeons to make it easier for you guys to do partial breast or planning treatment, target boost, whatever. So what do you think?
JOSHUA MONDSCHEIN: Well, I think all Dr. Rahimi's comments are really excellent. There was a recent editorial in the Journal of Clinical Oncology which basically discussed how, really nationwide, partial breast irradiation is underutilized. And I think there could be a number of reasons why. So I don't think there's just any one reason. But I think for patients who meet the ASTRO criteria, which we consider to be quote unquote "suitable" for partial breast irradiation, and, under the current guidelines, that's women 50 or older, typically T1 tumors, ER positive, excised with clear margins.
Probably the majority of these women should be getting or at least offered as a potential option, partial breast irradiation. And I think part of the reason why it's underutilized, I think, is, what I've heard when I've surveyed colleagues, is that there's sort of a low confidence, when they get a patient and do the planning scan, of exactly how to outline the cavity on a consistent basis. So I agree with Dr. Rahimi. I think any markers are good.
The issue is that there's a lot of variability, surgeon to surgeon, on how clips are left. And, also, the clips aren't really left in a perfect 3D pattern around the tumor. So it's hard for us to consistently outline where it was removed. So I think, by default, most radiation oncologists will go to whole breast radiation, because we know you're not going to miss your target. So I think that's kind of the heart of the issue.
ANTHONY LUCCI: I think that's actually really helpful information, because I know all of us have been guilty, in the past, of using clips, putting them around the margins, and then either we move tissue or the plastic surgery team move tissue, to a point where it may make it very difficult for you guys to really know what's going on. So, Karen, I think you were going to talk--
KAREN BARBOSA: Well, I can speak to that, because I think the thing is I'm at an institution where we use clips. And I think there's also a financial concern. And clips are what most people would be using. But what I'll say is that there are certain cases, like what Dr. Lucci was saying, where you're really going to need something like BioZorb to help you if you're going to keep the breast. And so I think trying to integrate it, and if you're at an institution that's using clips, maybe just trial it on a few of the larger cavities that you're doing, to bring it in for that. And then you'll see the utility.
So I just wanted, because I was looking at the poll and it looks like the majority of patients, not patients, sorry-- everyone's a patient to me-- the majority of attendees tonight are actually using clips. So I just wanted to address that, that at my current institution, we are using clips primarily. And then I'm trying to get them to let me use it on cases that I really need it.
ASAL RAHIMI: I mean, I wanted to make one more comment too. So this discussion doesn't just apply to partial breast. This also applies for the boost, which has been shown in several trials to have a local recurrence reduction when we do the boost. And so when some of these oncoplastics are done, and, even when clips are done, and, like we had mentioned before, they are all over the place, or we can't see them because reduction surgeries have been done and the clips have been removed, where we're removing a component of the oncological care and that's not good.
So we really need to make sure that cosmesis is very important, and I'm all about cosmesis. But it's also about curing the patients and giving them the best outcomes. So some type of localization is going to be very important just for the actual oncologic care of the patient.
ANTHONY LUCCI: I think that's a great comment, and I think really is helpful to us. And I have to admit, one of the reasons I started using BioZorb was because I really liked the ability to reconstruct large defects. But to know that it has that really big benefit for the radiation oncologist, I think adds a lot. Karen, I think you were going to talk a little bit more in detail about how much tissue we're moving. And for all of us, both surgeons, radiation oncologists, can you just talk a little bit more about the types of oncoplastic so we know what when we see an [INAUDIBLE] what we're looking at.
KAREN BARBOSA: Yeah, sure. I just wanted to say, if I could get control back of the screen, I'll move through it.
ANTHONY LUCCI: I can move it for you. I'll see.
KAREN BARBOSA: All right. So I mean I think this slide basically exemplifies the different patterns. But when we look at this slide, we have to understand the different levels. So let's move away from the minutia of the pictures to the bigger concept, which is which are the levels. So if we go to the next slide, we'll see the level 1 is less than 20% of the breast. So basically what we're doing is we're just simply reshaping, closing the cavity, and there's no skin excision.
You might be doing a little bit of a crescent lift, and that really is the most you want to move it, is about 3 centimeters. Plastic surgeons will gasp at the fact that you're doing a crescent, because the nipple areolar complex, known as the neck, has very soft tissue. And if you actually move it and you don't go circumferentially around the nipple, what's going to happen is you'll get a little football elongation of the neck. So you really don't want to use that too much.
But if they're going to get radiated, the radiation is actually your friend in this. And it'll actually tether down that breast tissue, so that you don't get a lot of that stretch that we would see if you didn't do that. And then, like I mentioned just now, is that if you go circumferentially all the way around, people will call it a Benelli, or a round block, or a donut, and basically that's going around the nipple completely and then creating a perimeter around that.
And that is basically going to keep it if there are two concentric circles, one and then another one around it, then your nipple will stay right where it is. If it's eccentric, it will lift it up or drop it down. And you can move it medial or lateral, if the tumor is on the medial or lateral side, to compensate for any radiation boost that you might be getting. But there are limitations to that procedure as well, because when you do too much of a circumferential change, basically you're flattening the breast form by narrowing the nipple areolar complex. With a vertical limb you can get it to actually look better.
But, for the most part, a simple, easy way to understand this is 20% of the breast or less is Level 1. Level 2 is more complex at 20% or greater. And I would say also depending on the size of the breast, right? So if you've got a B size breast, if it's a B cup, and you're taking out 20%, that could actually, even though it's only 20%, it can be, depending on what quadrant you're in, like I said, the upper inner is the most difficult to reconstruct, it can be a lot more challenging.
Basically when we're looking at 50%, we are looking at a large volume loss. And here, a lot of times, we're going to look to do skin removal. So those are times that you definitely want to incorporate a vertical mastopexy where you're going to take out tissue from below the nipple to tighten up that skin envelope. The way I describe this to patients and other doctors who were doing this when they're learning it for the first time, is if I have a pillow and I take out half that pillow, but I keep the same pillowcase, it's going to look terrible. Well, think of the pillow as the breast parenchyma, think of the pillowcase as the skin.
So if you're taking out the pillow, then you better take out some of the pillowcase so that like begets like and that the volumes match. So you really want a nice tight skin envelope over a nice tight breast. And that's where the volume replacement becomes really a critical issue and that's why I like to use the BioZorb. And then there's different techniques that you can use, mastopexy, which is raising the nipple, mammaplasty techniques like reduction.
And, once again, it's going to speak to your level of comfort. When I was in New York, my best friend was a plastic surgeon. We were Mutt and Jeff in the OR. And we would do these cases together. When I got to Alaska, the plastic surgeons didn't want to have anything to do with me. And I had patients who had either TRICARE or Medicare, and the plastic surgeons had the pick of the litter and I couldn't get anyone really to work with me. And so they would say, you do it, and on cases for recons, implants will be there.
So it was a really different spectrum and paradigm for me. And that's where I started doing more and more of this. And it's really about, one of the things is understanding what your comfort zone is. What is your facility with the procedures? What is your hospital like?
What are they going to let you do? What's your plastic surgeon availability? So working within your spectrum, just because other people are doing it, don't jump off the cliff. Make sure that you're ready to go before you jump.
So partnering with the plastic surgeon is a great way to get started, and, really, a way to avoid having a complication. I always say, if you're starting to do this for the first time, if you have a mistake, you're a butcher. If the plastic surgeon has a mistake or a complication, well, these things happen. So just to be aware that we're a little bit more under the microscope.
And I saw Dr. Lucci grinning under his beard. We can go to the next slide. And I think this is Josh.
JOSHUA MONDSCHEIN: Yeah.
KAREN BARBOSA: Taa-daa!
ANTHONY LUCCI: So Josh, can you enlighten us a little bit more about what are the kind of difficulties you have, and show us some of the issues regarding what you're planning when you're using, let's say, a seroma versus using a device that can actually outline the cavity. What do you got?
JOSHUA MONDSCHEIN: Sure. Yeah, it's a good question. So in terms of what the radiation oncologist has to use, if there is not a surgical cavity marker in place, really we're left with either using the seroma, or, potentially, if there are some surgical clips that are left behind.
And we know that these are very imprecise. There've been multiple papers written about this. But with seromas, the issue is that they can overestimate the size of the surgical cavity, because they can seep into surrounding tissues.
So when the radiation oncologist outlines the cavity, we actually wind up essentially irradiating more normal breast tissue than we'd like to. And the problem with clips is, again, they can migrate, so they're just not a reliable target, when you're trying to outline the cavity. So those are the two central issues that we see.
We see the next slide. And this is a slide looking at what modern 3D based treatment planning looks like for the radiation oncologist, with a BioZorb marker in place. So this is the first phase of radiation. This is a lady getting whole breast radiation, what we call tangent fields, where we're targeting the whole breast for the first phase of treatment. The majority of women will qualify for hypofractionated radiation therapy, which is traditionally given over the course of about three weeks.
And then like Dr. Rahimi mentioned, we can go to the next slide. The majority of women will qualify for a boost. A boost is essentially giving targeted radiation to the cavity itself to reduce the risk of local recurrence.
And this is a slide that demonstrates how that boost can be done rather nicely with a BioZorb in place, because you know exactly what you're treating. You could put a consistent margin on it. That can vary from institution to institution, or what protocol a patient's being treated on. Typically around the realm of 1 cm, but it depends on the protocol.
But at least with this you have a consistent marker in place for that boost phase.
ANTHONY LUCCI: So I'm just jump in and say I saw that there's a registry data that was published by Kaufman, I think it was Annals of Surgical Oncology, late last year, and I noticed they asked radiation oncologists, do you prefer having BioZorb versus not. I was actually shocked. I think it was like 87% said that it helped them with planning boost targets. So obviously that must be something very useful to have versus a bunch of clips kind of splayed out
KAREN BARBOSA: I was going to say, I actually work at a place where I have a very old radiation oncologist who's very old school and set in his ways. And this was actually the one thing that he actually had asked the university to bring to the system years ago. So just saying that I didn't believe it would be real, but yes.
ANTHONY LUCCI: So that registry was actually interesting. It also brought up another point, which you address, Karen, is always try to use one size smaller and cover with tissue. Because there was a mention of palpability, but when that was done it reduced again.
I think that's what I've noticed, talking to other surgeons, is one of the main reasons people are hesitant is they say, I've heard it can be palpable. But I've always tried to go a size smaller or even use the flap, 2 by 3 by 1, and just mark the bed with it and then pull some tissue over it. We still get great tissue replacement. But, sorry, I didn't mean to jump in the radiation oncology flow, but I think those are important points out of the registry data is to go with the smaller size and cover it. If you leave it right up near the skin, obviously, that's going to be a problem. Can I also ask Dr. Rahimi, what are your thoughts on the cavity size and--
ASAL RAHIMI: Yeah. No, I mean, I think that that's a perfect segue into what I wanted to discuss. So, I mean, treatment volume for radiation oncologists really matters, especially when we're doing sophisticated techniques like partial breast irradiation. So there are many different types of partial breast irradiation. One of the newer techniques that we have is called stereotactic partial breast irradiation.
And for those that are not familiar with that, it's basically doing less than five treatments, five treatments or less, of partial breast irradiation, and just using some different immobilization techniques, so we don't have to have these really large margins that we typically have to have with the external beam partial breast. But coming back to the point of the cavity size and having a smaller device, it's very important because we know that treatment volume for radiation, higher treatment volumes, larger treatment volumes basically correlates to higher toxicity.
And there's a direct correlation. And specifically from the press, it has been shown to correlate with higher rates of fat necrosis. So one of the trials that we had done, which was a stereotactic partial breast irradiation trial, found that this fat necrosis typically will develop in about 15% of patients. And it would happen at about one year. And it was directly correlated to the PTV volume, which is basically the volume that we're prescribing our dose to.
And the bigger the volume, the higher the incidence and the higher the percentage of fat necrosis development. And there was a cutoff at about 100 cc's, for really predicting for a higher probability of fat necrosis. So selecting a device that is as small as possible, so you can actually, in other words, shrink the cavity rather in comparison to just kind of leaving it open, would really help us radiation oncologists, because then we can have a smaller volume that we have to treat, which will then correlate to some of these other things that we were just mentioning.
So treatment volume matters for basically any type of partial breast irradiation, whether it's external beam, whether it's catheter-based, or stereotactic partial breast. So just kind of really quickly, just on the topic of the stereotactic partial breast, some of the other factors that we found that were associated with fat necrosis, if you move to the next slide, are women that have larger breasts were also associated with higher fat necrosis, and then people that got their fractions of radiation, when they're doing these stereotactic techniques, like on consecutive days, and just higher treatment, higher treatment prescription doses.
So if you go to the next slide, yeah, and this just shows the incidence of fat necrosis over time, with the median being around one year. But it can happen even out to like three years. So and when we're doing these partial breast techniques, it's really important to know what that is, so that we can first of all calm down the patients, and basically just document that with like an ultrasound, and continue to follow along.
But treatment size really does matter, and selection of a device that would actually reduce the cavity size, so that the radiation oncologist can treat a smaller volume is key.
ANTHONY LUCCI: Those are, I think, really great comments. One of the big things now for us as surgeons is, we really always want to offer breast conservation whenever possible, and some of the limitations before were, well, it may not look good. Like Karen said, you take half the pillow away, the pillowcase doesn't fit. I actually use the same analogy. That's a great analogy, but you're taking out the pillow, you need the case.
So I think it's been interesting because now we're always looking for ways to de-escalate therapy, de-escalate radical surgery, be able to extend breast conservation. So I just wanted to point out, one of the other things that we haven't talked yet, but is localization. So when we're talking about localization, we've talked about seeds, or whatever. There's many different ways, wires. People have used wires.
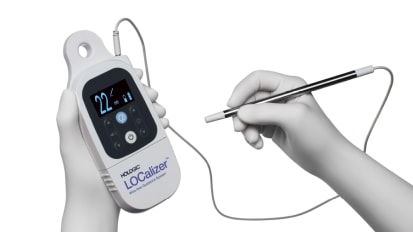
One of the things we've done and I've really liked using is the localizer. And I have to say that the, really, I think, big benefit that I've seen is that when each of your RFID markers, especially if you're bracketing a lesion, when you place the probe over the marker, you get a unique RFID signal. So this, I think, illustrates that. This was a lesion that was bracketed. And so when you place your probe over each marker, you get a code that tells you which is the anterior marker, which is the posterior marker.
Or let's say you have three. Sometimes we had three, even four. It may tell you which is the medial or lateral. So you actually know which way you're going and which marker you're going after. Sometimes when you don't have a unique identifier, especially if the markers are close, now these markers are fairly close and that's why I want to point out, we actually, when we did the case, you could really tell which one was which, which was your anterior, which was your posterior, because you're getting a unique RFID signal.
So I found I'll look at the poll and see what the different people, what different modalities people are using. But I found that to be really useful. And, Karen, I know you're going to talk about a case of breast conservation. I think we can segue right into that, and we'll talk more about this as we go on about different localization techniques.
KAREN BARBOSA: Yeah, I think that this is a great example. And I think this is also very poignant, because this is one of my first cases that I did. I had brought the BioZorb out to Alaska and championed it for my patients. She had a probably B/C cup, not a very large breast.
As you can see, she's got some ptosis going on. And she had two biopsies done, which were both returned as cancer, basically at the 12 o'clock and the 1 o'clock. So they weren't really weren't that close or far from each other. But they felt that these were two separate lesions.
When I look at them and they had the sizing of about 2.6 centimeters, and the other one being 1.7, I felt they were so close, clockfaces, that they were actually one large unit ER/PR positive, HER2 negative. She was BRCA negative and clinically node negative. She was very concerned about fertility and really was a young woman and wanted to make sure that she could keep her breasts.
So if we go to the next slide, what I recommended was neoadjuvant to shrink the tumors due to the size, and the upper inner quadrant was the location, so we really didn't have much to work with. When is a positive margin a good thing? When you're first starting off with BioZorb and you place a spiral, thinking that you're marking the two tumors that you thought were all one tumor in the upper inner quadrant.
Well, luckily we got a positive margin, and I got to take her back and redo what I had done. I went back. I took a re-excised margin. It was nice, because it actually turned out to be negative. But I dropped too low profiles in the upper inner quadrant, and I rotated a flap of tissue over that area.
So when we did it, it gave me the opportunity to re-evaluate what was going on. And clinically she couldn't feel it anymore. And we marked a tumor bed appropriately, because they were, on pathology, two distinct tumors, and the re-excision margin was indeed negative, as is usually the case.
Let's go to the next slide. And this was her post op picture, where she was really now loving her cancer breast but not loving her native breast. And she complained that she didn't like her native breast. So she was also military and wanted to stay in the area and didn't want to get PS'ed out to another location. So she used her need to stay with her oncoplastic surgeon in Alaska for symmetry.
So she waited a year for the radiation changes to settle. And then we went back and we did a vertical mastopexy on the contralateral side. So if we go to the next slide I'll show you that. Here it is. I basically did a vertical mastopexy. The middle picture is what I call the double bubble, taking that de-epithelialized ring above the nipple, and taking that de-epithelialized flap of tissue below the nipple, basically is closing that pillowcase.
The inferior pole is now being tightened up and pushing tissue into the upper quadrant, which if you look at her first picture on this slide, you can see she's really flat here. And on the other side it looks like she's got an implant. In fact, when I asked my plastics friends what to do with her, they said just use the same size implant. Anyway, when we did her symmetrization, we did the vertical mastopexy, pushing the tissue up, tightening up the skin envelope in the lower pole.
And if we go to the next slide, we'll see that she had a pretty good symmetry, with her nipples being at the same level. And this is pretty much, I think, about three weeks post-op, so she's got a little bit of post-op swelling. And you can still see her scar lines pretty prominently. And those will fade over time.
She was incredibly happy with her scar, and her cosmetic outcome. And it really marked the tumor bed well. So we can go to the next slide, I think, and pass this off to our pal, Dr. Rahimi.
ASAL RAHIMI: Yeah, thank you. So, yeah, well, thank you, that was a very nice example. So really, I mean, just to make sure all the viewers are really understanding how much this device can be so good for us is that, I mean, it really serves as a marker for the surgeon and the radiation oncologist. So we can communicate with each other and really know where we need to target, and then, on top of that, also kind of helping collapse the cavity, so that we can have smaller volumes to treat.
So here is an example, on the left side where we're using a 2 by 2 centimeter device. And then the radiation oncologist treatment volume after doing all of our margin enlargements is about 57 cc's versus a similar case that just has the clips placed. The PTV volume, the treatment volume, is much more difficult to discern.
You can kind of see the one clip there, but it's hard to know where the edges are. And the volume is twice as large. It's 121 cc's. I mean obviously this is not the same patient. But that kind of just gives a sense of, from a radiation oncology perspective, how this all ties in.
ANTHONY LUCCI: Very nice. I think that really illustrates that fact. So let's talk a little bit about, and, again, I think this is obviously a timely issue, but can you just comment a little bit on what's been, about partial breast, and especially now with all of us facing issues about, can we access the OR, can we get patients in? How do we maximize resource use during radiation? Could you comment a little bit about that?
ASAL RAHIMI: Yeah, so I think that back in March when the COVID pandemic really hit and everything was just kind of shut down, there were a lot of trends that we had seen, and I think as a field everybody had seen. And so one was the conservation of PPE, and two, the resources, including the operating room, and just the personnel and reducing exposures.
And so there were several manuscripts that came out about breast radiation oncology at this time, and giving some guidelines as far as what we should be doing in this type of era. And also I think they commented on surgical issues as well. And so some of the things that were commented on were really kind of discouraging, the use of brachytherapy at the time.
If your particular hospital had a surge and didn't have enough PPE and didn't have the personnel, and you're trying to reduce exposure risks, to really take a second thought about doing brachytherapy, and, if you're going to do partial breast, to actually do more of like the external beam, because it would help with those particular resources. And also there could be potential reduced infection rates.
So that was the first thing. And then the second thing was, really for this early stage breast cancer, like suitable criteria is really trying to do partial breast for those patients and also doing a lot more neoadjuvant endocrine therapy to postpone the actual surgery so that we could utilize those ORs for other situations. But trying to offer those patients partial breast irradiation rather than doing whole breast irradiation, in the situation of COVID, one, to reduce exposure for patients coming into the radiation oncology suite and waiting in waiting rooms, and so they would have less trips.
And we would have less people coming in and out of the radiation oncology suite. And then, two, just kind of more of a convenience, and then, three, reducing PPE if you're not doing brachytherapy and doing external beam partial breast irradiation techniques. And then we mentioned the neoadjuvant endocrine therapy to try to help postpone the surgery if necessary, if your particular hospital required that.
There are several different ways that partial breast irradiation can be done with an external beam technique. There's a 38.5 gray and 10 fraction BID technique that was published up to 10 years in the RAPID trial and then it's ABP 39. However there was some issues with cosmesis in those studies. So that is, if you are going to use that regimen and use a BID fractionation, it is definitely urged that you discuss cosmetic outcomes with the patients.
There have been several other regimens that have showed better cosmetic outcomes, including a 40 gray 10 fraction or a 30 gray in 5 fraction technique at the University of Florence. And that was published in the phase three clinical trial using IMRT as their technique, which actually showed very good cosmesis.
So there are different options, and different practitioners are going to have a different comfort level with each of these different fractionations. But these are things that we should really think about in the COVID pandemic and being able to offer these to our patients.
ANTHONY LUCCI: So can I ask you guys about, has bundling of payments had any effect on your treatment planning? Dr. Mondschein or Dr. Rahimi?
JOSHUA MONDSCHEIN: I think the alternative payment model RO-APM is new. I mean, basically this has rolled out recently, and in certain areas it's being delayed. But I think most audience members will be familiar. But the general concept is that providers or hospital systems will be paid a set professional fee and a set technical fee, regardless of what modality they choose to use.
So, essentially, what this is likely born out of is that, for years, there have been some centers that have essentially potentially put up patients on treatment plans which required essentially more fractions or more treatments. And the idea is, the point of this payment model is to really incentivize health care systems and providers to choose the most appropriate regimen for their patients.
So I think, to answer the question, it's been out for such a short period of time that, well, it'll take time to be able to survey providers to see how this has changed practice. But I think it will certainly push people in the right direction of thinking of how to stay within guidelines in treating patients with the most appropriate regimen based on their pathology and tumor type.
ANTHONY LUCCI: Great. Dr. Rahimi, did you want to say something? I'm sorry.
ASAL RAHIMI: Yeah, I mean, I would just add that I think that the trend is going to be that we're seeing is to do these shorter fractionation courses for many different sub-sites in the body as far as radiation oncology. I mean even in Europe, they've recently published doing whole breast radiation in five treatments. So these are things that we're going to be seeing as more trends.
A lot of people are now doing Canadian fractionation. So they're doing 15 or 16 treatment fractions. And then, even with the partial breast, I mean, we have a clinical trial where we're doing one fraction, and that's been done quite commonly in Europe and some of the other institutions that have intraoperative radiation. But we can now do that with stereotactic partial breast.
So I think the trend is doing less is more, and if it's just as effective, then why not offer that to our patients. It's more convenient for patients, and it has less strain on hospital systems. And now with the COVID pandemic that all of that has just ballooned. It's just that's more convenient for everybody at this point.
ANTHONY LUCCI: Yes. So we have five minutes to the hour. I just want to make sure if there's any attendees that had any questions. Or Macey, do we have any questions that have been posed? I would hope we could answer those before the hour.
MACEY NELSON: Yeah, we do. So first of all, let me just say thank you to the four of you for leading us through a really fantastic conversation. I think you addressed a lot of the questions that were coming in from our audience. But there are a few that I saved to the end. And the first actually would be posed to the two surgeons. So, when you're moving a lot of tissue and doing tissue transfers, how do you handle a positive margin?
ANTHONY LUCCI: Karen, do you want to go first?
KAREN BARBOSA: Yeah, sure. I think the thing is the sooner you can go back, the better, because what will happen is you can basically unravel the rolls that you've placed. And what I try to do is just pop the sutures like with a knife gently, just open it up, and then go down. Since it's fresh, the sutures haven't really embedded. They haven't dissolved yet. You can find your way back.
And then since you placed it yourself, you know where to go. So I don't think it's a contraindication when you're moving tissue. And it's helpful, like I said, if you document things in your op note, like I said, what size BioZorb you use. How did you rotate this flap? Just so that you have a way to find your way back. But the sooner you go back is the really big helpful tip.
MACEY NELSON: Yeah.
ANTHONY LUCCI: I would say that, yeah, and I would say the best way to deal with it is to try to not have one. But to do that involves a time investment up front. And so what we do is we actually do specimen radiographs. We do whole specimen, then we do slice specimen radiographs. The radiologist looks at each slice specimen and tells us if there's any density, any abnormality, anything near any of the margins.
We would take that during the case. And the pathologist then is also looking grossly to make sure there's nothing. Now this all takes time. But I think that investment in time has resulted in us having an extremely low margin positivity rate.
So that, I don't want to jinx anything, but I don't remember. So it's been really fortunate. That doesn't happen often. So it's an investment up front to avoid it down on the back side. Some people would rather not send it and do that.
I understand that, but I actually think the best way is to try not to have one. And when you do, I agree with what Karen said, go back. And if the BioZorb is completely covered and away from the area, oftentimes you can leave it in place. But that's the whole point of putting the tissue over it and putting it deeper, not right under the skin.
MACEY NELSON: Yeah.
KAREN BARBOSA: I think it's important to understand that every facility or hospital has different abilities. I use intraoperative imaging as well. And having these surgical oncology techniques, such as oncoplasty, really does limit, because it makes you able to take more tissue. So a positive margin just by having oncoplastic in your back pocket, really allows you to take more tissue and recreate the cavity, so that you do get less margins.
But for those of you if you do have a positive margin don't be afraid. It's not a contraindication. And the tip is really go back sooner rather than later. But like Dr. Lucci, when you do intraoperative imaging, your re-excision rates really drop dramatically. It's hugely helpful.
ANTHONY LUCCI: And actually you bring up a good point. The whole reason I started using BioZorb was because I needed something to fill in the space, because I wanted to be able to do larger lumpectomies. And even if you're going to do an adjacent tissue transfer, some really simple technique, adding that in made it so much easier to replace the volume. So I'm glad it's providing benefit to the radiation oncologist as well. But our selfish reason was because we could make the breast look better. That's the honest answer.
KAREN BARBOSA: Funny because this was my eye-opening, that you guys actually liked it. Like I said, when my rad-onc, who was really old school and actually paper charting, said, I wanted this years ago, it was an eye opener.
And then when we had the discussion about putting this panel together, I was like, you guys actually really like it? Is it that important to you? I was doing it because I was being selfish. I wanted great outcomes for my patients. I wanted to look like a stud as a surgeon. What surgeon doesn't want that?
And I think patients really do benefit by having a lesser surgery. Going to mastectomy just because you can't make the breast look like a breast is really more of a disservice to patients. Complications with contracture can be an issue, loss of sensation, it doesn't always last. Implants sometimes need to get replaced after years. So I think the more we pro-game with trying to keep a woman's breast is the best plan.
MACEY NELSON: Wonderful. Well, listen. We are coming up to the very top of the hour. For those of you that did put a question into our question box, thank you so much. If we didn't get an opportunity to answer it, trust me, we will answer it via email after the completion of the program. I just want to say, thank you, to everyone for participating. A huge thank you for our four panelists. It has been a pleasure listening to all of you talk.
And I will say for our audience members, if you would like additional medical education offerings, please do visit HologicEd.com and it has, again, just been our pleasure. Thank you so much. Enjoy the rest of your evening.
ANTHONY LUCCI: Thank you everyone.
JOSHUA MONDSCHEIN: Thank you.
ASAL RAHIMI: Bye.
KAREN BARBOSA: Thank you.
MACEY NELSON: Stay safe.
Sharing Perspectives on the Reconstructive Lumpectomy: A Discussion for Surgeons and Radiation Oncologists
Originally Broadcast: Thursday, January 21 at 4PM PST (7PM EST)
An interactive, case-based panel discussion designed to:
Participants will have an opportunity to ask questions and hear about the latest breast reconstruction methods from a multi-disciplinary team, including two surgeons and a radiation oncologist, practicing in both Academic and Community based centers.
Tips & Tricks
Related Presenters

Breast Surgeon, University of Maryland Shore Regional Health

Breast Surgeon, MD Anderson Cancer Center, Department of Breast Surgical Oncology, University of Texas

Radiation Oncologist, Tennessee Oncology / Provision Proton Therapy center, Nashville, TN

As Associate Professor of Radiation Oncology at UT Southwestern Medical Center, Asal Rahimi, M.D., M.S., says she is doing exactly what she was trained to do: she is using radiation therapy to treat breast cancer patients. After receiving ...
Related Videos